

The use of pluripotent stem cells to generate diagnostic tools for transfusion medicine
- PMID: 35977098
- PMCID: PMC9707399
- DOI: 10.1182/blood.2022015883
The use of pluripotent stem cells to generate diagnostic tools for transfusion medicine
Abstract
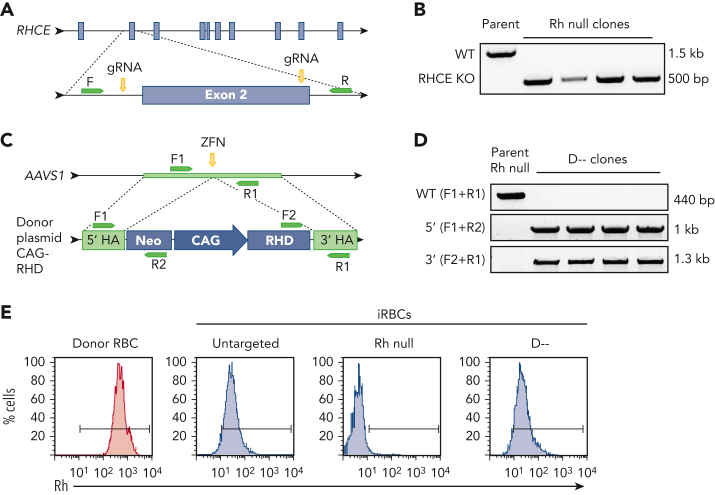
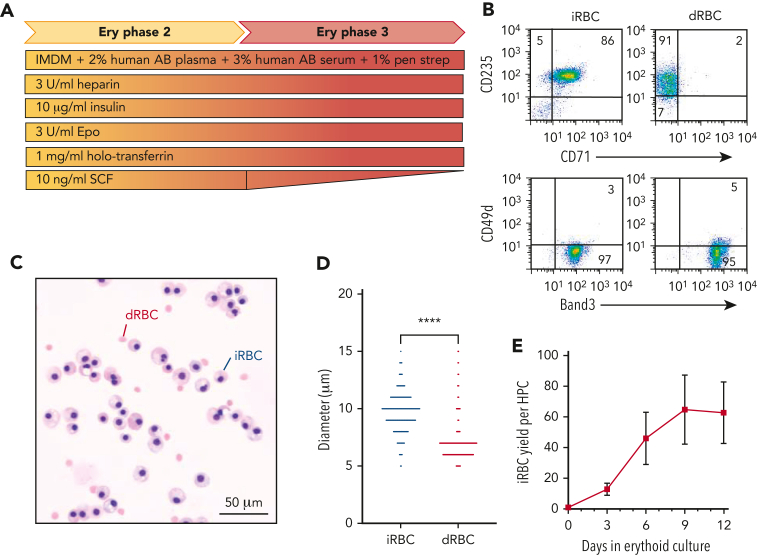
Red blood cell (RBC) transfusion is one of the most common medical treatments, with more than 10 million units transfused per year in the United States alone. Alloimmunization to foreign Rh proteins (RhD and RhCE) on donor RBCs remains a challenge for transfusion effectiveness and safety. Alloantibody production disproportionately affects patients with sickle cell disease who frequently receive blood transfusions and exhibit high genetic diversity in the Rh blood group system. With hundreds of RH variants now known, precise identification of Rh antibody targets is hampered by the lack of appropriate reagent RBCs with uncommon Rh antigen phenotypes. Using a combination of human-induced pluripotent stem cell (iPSC) reprogramming and gene editing, we designed a renewable source of cells with unique Rh profiles to facilitate the identification of complex Rh antibodies. We engineered a very rare Rh null iPSC line lacking both RHD and RHCE. By targeting the AAVS1 safe harbor locus in this Rh null background, any combination of RHD or RHCE complementary DNAs could be reintroduced to generate RBCs that express specific Rh antigens such as RhD alone (designated D--), Goa+, or DAK+. The RBCs derived from these iPSCs (iRBCs) are compatible with standard laboratory assays used worldwide and can determine the precise specificity of Rh antibodies in patient plasma. Rh-engineered iRBCs can provide a readily accessible diagnostic tool and guide future efforts to produce an alternative source of rare RBCs for alloimmunized patients.
© 2022 by The American Society of Hematology.
Conflict of interest statement
Figures





Comment in
-
Precision transfusion medicine: a new spin.Blood. 2022 Oct 13;140(15):1661-1663. doi: 10.1182/blood.2022018080. Blood. 2022. PMID: 36227750 No abstract available.
References
-
- Nickel RS, Hendrickson JE, Fasano RM, et al. Impact of red blood cell alloimmunization on sickle cell disease mortality: a case series. Transfusion. 2016;56(1):107–114. - PubMed
-
- Noizat-Pirenne F, Tournamille C. Relevance of RH variants in transfusion of sickle cell patients. Transfus Clin Biol. 2011;18(5):527–535. - PubMed
-
- Chou ST, Jackson T, Vege S, Smith-Whitley K, Friedman DF, Westhoff CM. High prevalence of red blood alloimmunization in sickle cell disease despite transfusion from Rh-matched minority donors. Blood. 2013;122(6):1062–1071. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
