

Association Between Medicaid Prescription Drug Limits and Access to Medications and Health Care Use Among Young Adults With Disabilities
- PMID: 35977173
- PMCID: PMC8796920
- DOI: 10.1001/jamahealthforum.2021.1048
Association Between Medicaid Prescription Drug Limits and Access to Medications and Health Care Use Among Young Adults With Disabilities
Abstract
Importance: Prescription drugs are necessary for managing complex physical and mental health conditions for more than 10 million Medicaid beneficiaries with disabilities. However, some state Medicaid programs limit the number of prescription drugs that beneficiaries can obtain monthly, which may decrease access to essential medications.
Objective: To examine the association between exposure to the 3-drug limit at age 21 years in Arkansas and Texas and prescription drug and health care use among beneficiaries with disabilities enrolled in Medicaid.
Design setting and participants: In this cohort study of 28 046 young adults with disabilities, difference-in-differences analysis was performed using Medicaid Analytic eXtract claims data from January 1, 2007, to December 31, 2012. Analyses were completed December 1, 2020. The analyses included Medicaid beneficiaries with disabilities in Arkansas and Texas (ie, drug cap states) or 15 comparison states without drug cap policies who became age 21 years during the study period and were continuously enrolled in fee-for-service Medicaid in the year before and after that point.
Exposures: Exposure to the 3-drug prescription limit at age 21 years in 2 drug cap states.
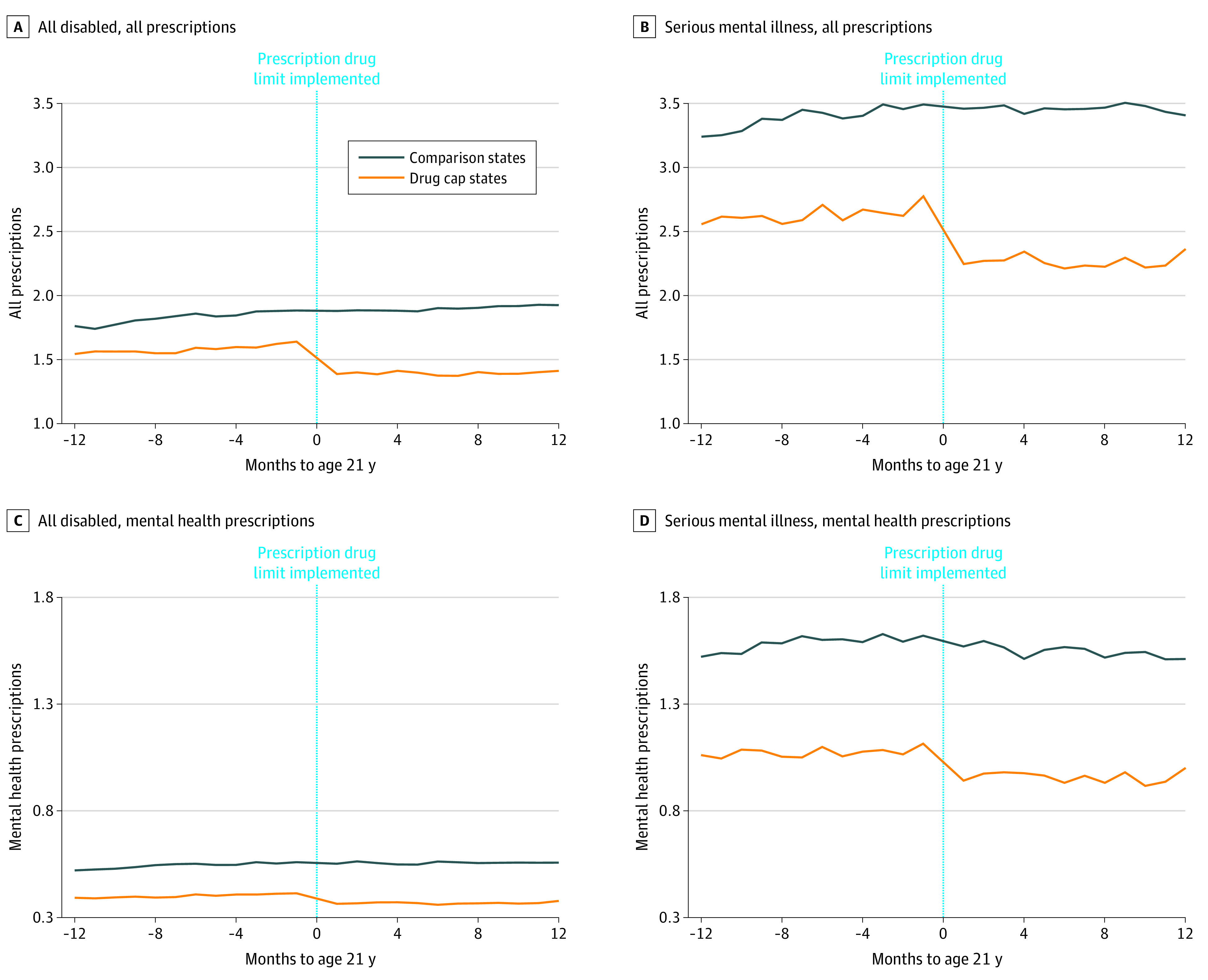
Main outcomes and measures: Monthly total prescriptions and prescriptions for drugs to treat mental health conditions, total prescription drug spending, and inpatient and emergency department visits and spending in the 12 months before and after becoming age 21 years.
Results: Among 28 046 young adults with disabilities, 8214 (29.3%) resided in drug cap states and were subject to the 3-drug limit at age 21 years. Most individuals were male (drug cap states: 61.4%, comparison states: 60.6%), and the minority were White individuals (drug cap states: 36.7%, comparison states: 49.4%). More than one-half of individuals with disabilities were diagnosed with a mental health condition before age 21 years (drug cap states: 57.0%, comparison states: 60.0%). In the year before the analyzed individuals became aged 21 years, the mean (SD) number of prescriptions per beneficiary per month was 1.58 (2.16) in drug cap states vs 1.82 (1.91) in comparison states. The drug cap policy was associated with 19.6% (95% CI, -21.3% to -17.8%; P < .001) fewer monthly prescriptions and 16.5% (95% CI, -21.9% to -10.8%; P < .001) fewer prescriptions for drugs for mental health conditions but was not associated with total prescription drug spending. The drug cap policy was associated with 13.6% (95% CI, 1.9% to 26.6%; P = .02) more inpatient admissions.
Conclusions and relevance: In this cohort study of young adults with disabilities, drug cap policies were associated with lower rates of access to important medications and higher rates of hospitalization among individuals in states with drug cap policies vs those without these policies.
Copyright 2021 Geiger CK et al. JAMA Health Forum.
Conflict of interest statement
Conflict of Interest Disclosures: Dr Geiger reported being currently employed by Genentech. Dr Sommers reported receiving personal fees from Health Research & Educational Trust Stipend for the editor's position at Health Services Research, grants from Baylor Scott & White, personal fees from Massachusetts Medical Society honorarium for lecture, honorarium from Urban Institute for grant review, honorarium from AcademyHealth for grant review, honorarium from American Economics Journal for journal review, consulting fees from the Illinois Department of Healthcare and Family Services, and grants from the Commonwealth Fund and the Robert Wood Johnson Foundation outside the submitted work; Dr Sommers is currently on leave from Harvard and serving in the US Department of Health and Human Services. However, this article was conceived and drafted while Dr Sommers was employed at the Harvard School of Public Health, and the findings and views in this article do not reflect the official views or policy of the US Department of Health and Human Services. No other disclosures were reported.
Figures
Comment in
-
Three Decades of Drug Cap Studies Are Enough.JAMA Health Forum. 2021 Jun 4;2(6):e211249. doi: 10.1001/jamahealthforum.2021.1249. JAMA Health Forum. 2021. PMID: 36218757 No abstract available.
Comment on
-
Self-reported Behaviors Regarding Medications to Save Money Among Sexual Minority Adults in the US, 2015-2018.JAMA. 2021 Dec 28;326(24):2526-2529. doi: 10.1001/jama.2021.20335. JAMA. 2021. PMID: 34962541 Free PMC article.
References
-
- MACPAC: Medicaid and CHIP Payment and Access Commission. People with disabilities. 2017. Accessed October 14, 2020. https://www.macpac.gov/subtopic/people-with-disabilities/
-
- Kronick RG, Bella M, Gilmer TP, et al. The Faces of Medicaid III: Refining the Portrait of People With Multiple Chronic Conditions. Center for Health Care Strategies Inc; 2009:1-30.
-
- Bagchi A, Verdier J, Esposit D. Chartbook: Medicaid pharmacy benefit use and reimbursement in 2009. Mathematica Policy Research. December 12, 2012. Accessed February 1, 2019. https://www.mathematica.org/-/media/publications/pdfs/health/chartbook20...
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
