

Association of Medicare Advantage Star Ratings With Racial, Ethnic, and Socioeconomic Disparities in Quality of Care
- PMID: 35977175
- PMCID: PMC8796982
- DOI: 10.1001/jamahealthforum.2021.0793
Association of Medicare Advantage Star Ratings With Racial, Ethnic, and Socioeconomic Disparities in Quality of Care
Abstract
Importance: Medicare Advantage (MA) plans, which disproportionately enroll racial/ethnic minorities and persons with socioeconomic disadvantage, receive bonus payments on the basis of overall performance on a 5-star rating scale. The association between plans' overall quality and disparities in quality is not well understood.
Objective: To examine the association between MA star ratings and disparities in care for racial/ethnic minorities and enrollees with lower income and educational attainment.
Design setting and participants: This cross-sectional study included 1 578 564 MA enrollees from 454 contracts across the 2015 and 2016 calendar years. Data analyses were conducted between June 2019 and June 2020.
Exposures: Self-reported race and ethnicity and low socioeconomic status (SES) (defined by low income or less than a high school education) vs high SES (neither low income nor low educational attainment).
Main outcomes and measures: Performance on 22 measures of quality and satisfaction determined at the individual enrollee level, aggregated into simulated star ratings (scale, 2-5) stratified by SES and race/ethnicity.
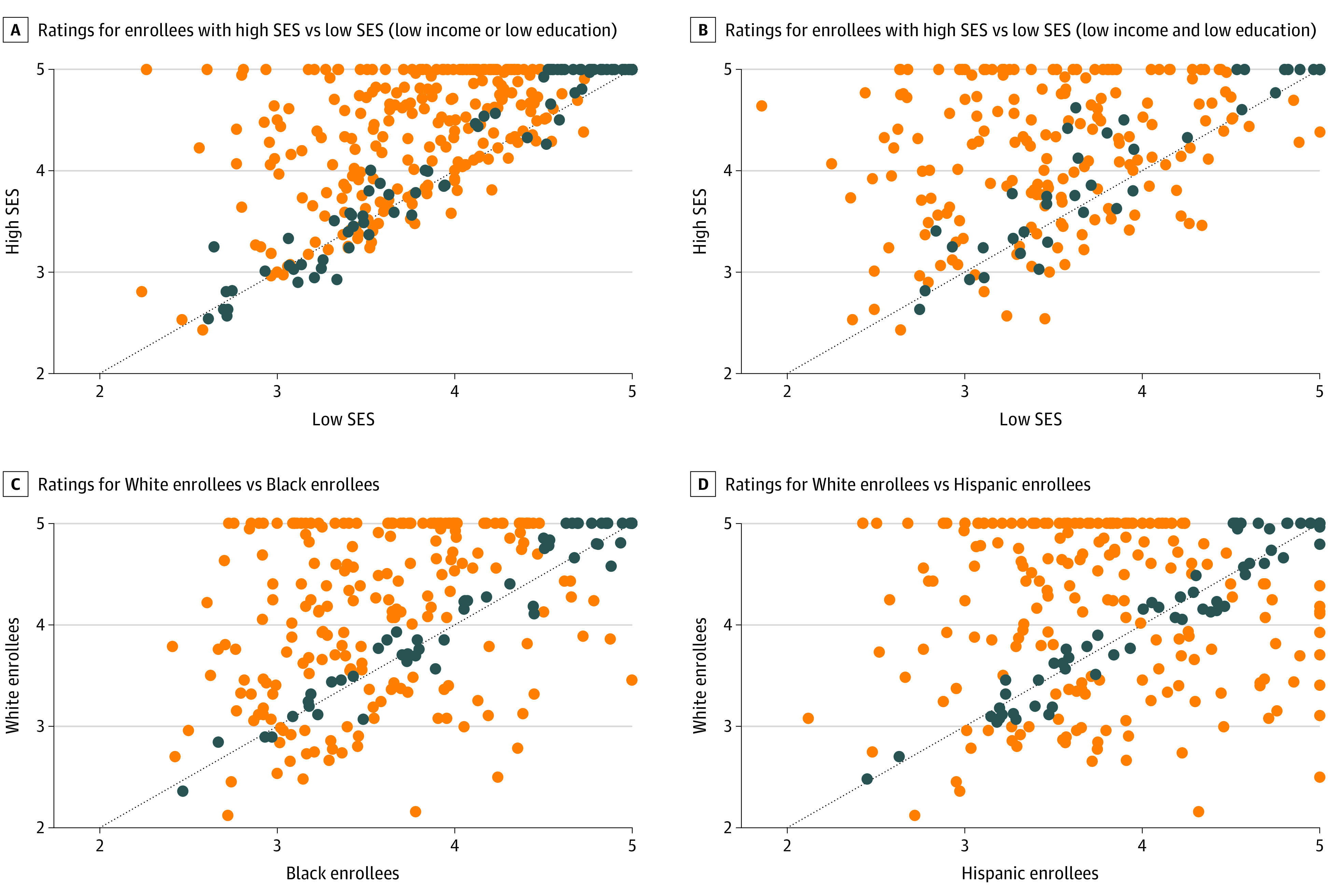
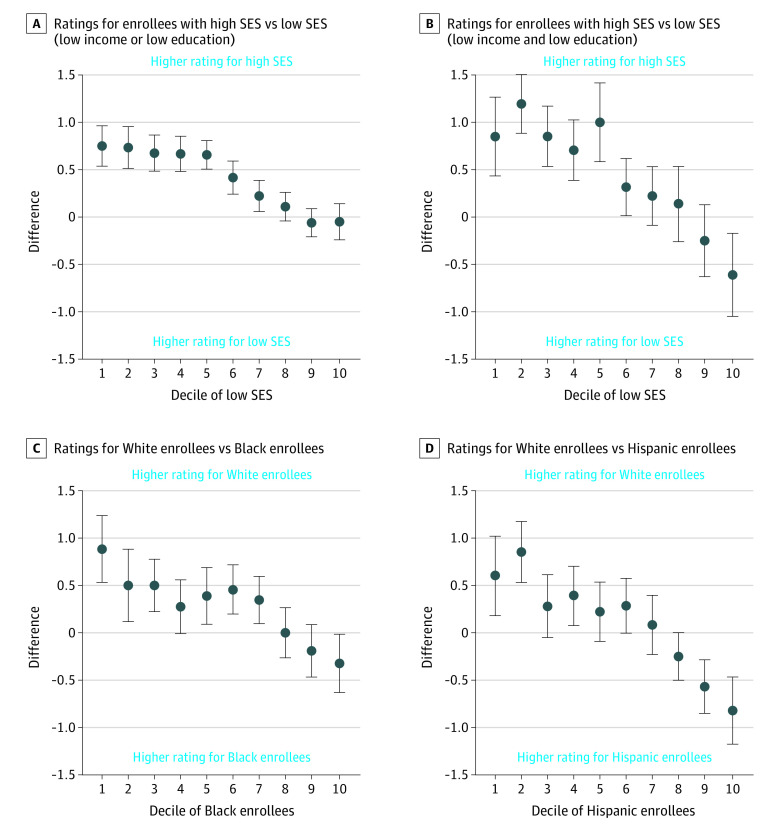
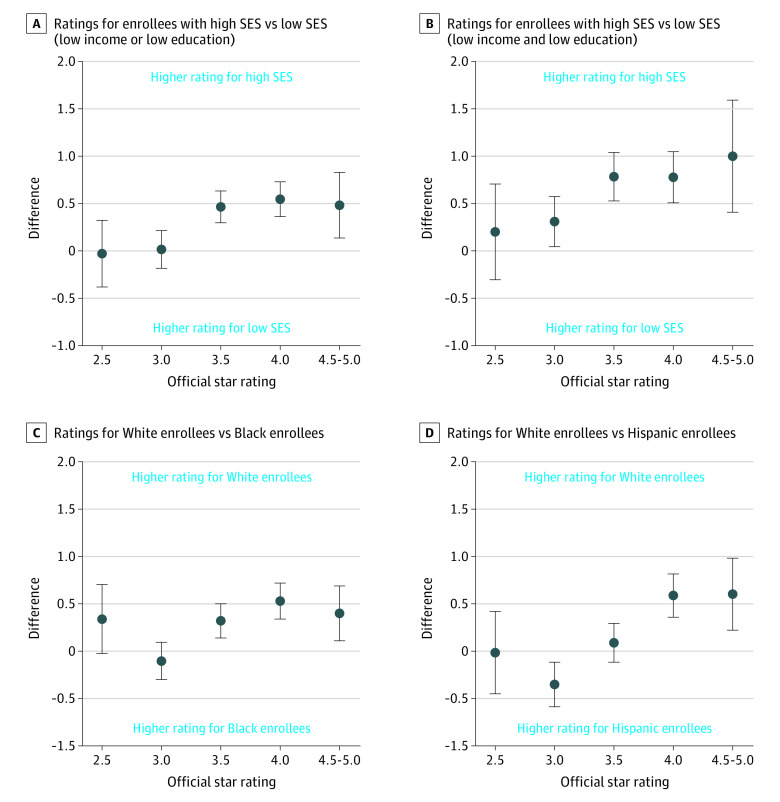
Results: A total of 1 578 564 enrollees were included in this analysis (55.8% female; mean [SD] age, 71.4 [11.3] years; 65.8% White; 12.3% Black; 14.6% Hispanic). Enrollees with low SES had simulated stratified star ratings 0.5 stars lower (95% CI, 0.4-0.6 stars) than individuals with high SES in the same contract. Black and Hispanic enrollees had simulated star ratings that were 0.3 stars (95% CI, 0.2-0.4 stars) and 0.1 stars (95% CI, -0.04 to 0.2 stars) lower than White enrollees within the same contracts. Black enrollees had a 0.4-star lower rating (95% CI, 0.1-0.7 stars) in 4.5- to 5-star contracts and a no statistical difference in 2.0- to 2.5-star-rated contracts (difference, 0.3 stars; 95% CI, -0.02 to 0.7 stars). Hispanic enrollees had a 0.6-star lower simulated rating (95% CI, 0.2-1.0 stars) in 4.5- to 5-star contracts and no statistical difference in 2- to 2.5-star contracts (difference, -0.01 stars; 95% CI, -0.5 to 0.4 stars). There was low correlation between simulated ratings for enrollees of low SES and high SES (difference, 0.2 stars; 95% CI, 0.03-0.4 stars) and between simulated ratings for White and Black enrollees (difference, 0.4 stars; 95% CI, 0.3-0.5 stars) and White and Hispanic enrollees (difference, 0.3 stars; 95% CI, 0.2-0.4 stars). As the proportion of Black and Hispanic enrollees increased in a contract, racial/ethnic disparities in ratings decreased.
Conclusions and relevance: In this cross-sectional study, simulated MA star ratings were only weakly correlated with those for enrollees of low SES in the same contract, and contracts with higher star ratings had larger disparities in quality. Measures of equity in MA plans' quality of care may be needed.
Copyright 2021 Meyers DJ et al. JAMA Health Forum.
Conflict of interest statement
Conflict of Interest Disclosures: Dr Meyers reported receiving grants from the Agency for Healthcare Research and Quality during the conduct of the study and personal fees from NORC outside the submitted work. Dr Rahman reported receiving grants from the National Institute on Aging during the conduct of the study. Prof Mor reported receiving grants from the National Institute on Aging during the conduct of the study, receiving personal fees as the chair of the scientific advisory committee at naviHealth Inc, and is the former chair of the independent quality committee at HCR ManorCare and former director of PointRight Inc, where he holds less than 1% equity. Dr Wilson reported receiving grants from the National Institute of Mental Health during the conduct of the study. Dr Trivedi reported receiving grants from the National Institute on Aging during the conduct of the study and grants from the Agency for Healthcare Research and Quality outside the submitted work.
Figures
Comment in
-
Opportunities to Address Health Disparities in Performance-Based Accountability and Payment Programs.JAMA Health Forum. 2021 Jun 4;2(6):e211143. doi: 10.1001/jamahealthforum.2021.1143. JAMA Health Forum. 2021. PMID: 36218754 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
