Association of Patient Race and Ethnicity With Differences in Opioid Prescribing by Primary Care Physicians for Older Adults With New Low Back Pain
- PMID: 35977182
- PMCID: PMC8796941
- DOI: 10.1001/jamahealthforum.2021.2333
Association of Patient Race and Ethnicity With Differences in Opioid Prescribing by Primary Care Physicians for Older Adults With New Low Back Pain
Abstract
Importance: Substantial patient racial and ethnic differences in opioid prescribing have been documented, but how much of these differences were attributable to physicians prescribing opioids differently to patients of racial and ethnic minority groups is unknown, particularly during the first wave of the opioid epidemic when the dangers of opioid prescribing and use were not as well known.
Objective: To examine associations of patient race and ethnicity with differences in opioid prescribing by the same primary care physician (PCP) for new low back pain episodes among older adults from 2007 to 2014.
Design setting and participants: This cross-sectional study used Medicare data of PCP office visits by Medicare beneficiaries who were 66 years or older with new low back pain.
Main outcomes and measures: Prescribing of any opioid in the first year of a new low back pain episode (days 1-365) and subsequent long-term use of an opioid (prescribed for ≥180 days in days 366-730).
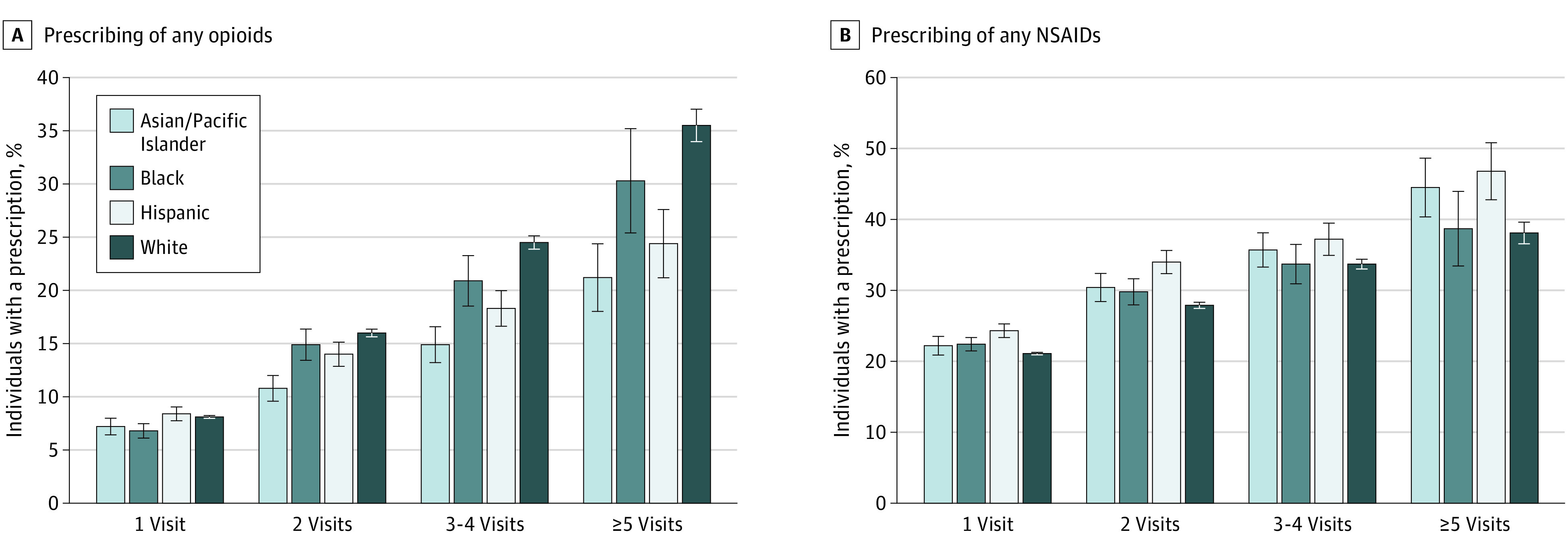
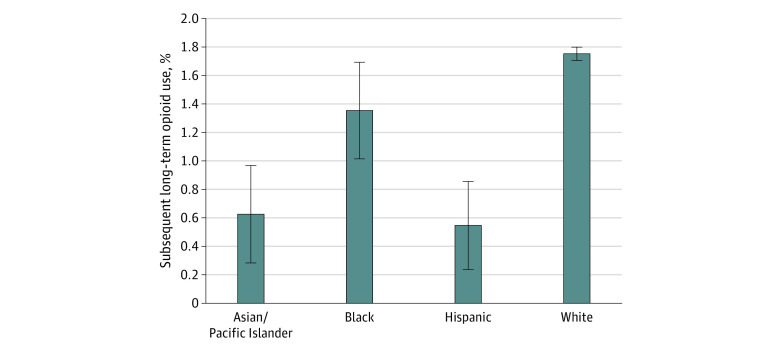
Results: Among the study population of 274 771 patients (mean [SD] age, 77.1 [7.2] years; 192 105 [69.9%] women) with new low back pain, 15 285 (6%) were Asian or Pacific Islander, 16 079 (6%) were Black, 21 289 (8%) were Hispanic, and 222 118 (81%) were White, cared for by 63 494 physicians. In adjusted analysis, on average, 11.5% of the White patients (95% CI, 11.4 to 11.6) received an opioid prescription in the first year of new low back pain. The same prescribing physician was 1.5 percentage points (PP; 95% CI, -2.2 PP to -0.8 PP) less likely to prescribe an opioid if the patient was Black, 2.7 PP (95% CI, -3.5 PP to -1.8 PP) less likely if the patient was Asian or Pacific Islander, and 1.0 PP (95% CI, -1.7 PP to -0.3 PP) less likely if the patient was Hispanic. The same physician was more likely to prescribe a prescription nonsteroidal anti-inflammatory drug to a patient of a racial or ethnic minority group. White patients with new low back pain were more likely to develop subsequent long-term opioid use than patients of racial and ethnic minority groups (eg, 1.8% for White patients vs 0.5% for Hispanic patients).
Conclusions and relevance: This cross-sectional study found that from 2007 to 2014, primary care physicians prescribed opioids for new low back pain more often to White patients than to patients of racial and ethnic minority groups. These results suggest that there may have been unequal treatment of pain by physicians when less was known about the morbidity associated with opioid use.
Copyright 2021 Ly DP. JAMA Health Forum.
Conflict of interest statement
Conflict of Interest Disclosures: None disclosed.
Figures