

COVID-19-Related Insurance Coverage Changes and Disparities in Access to Care Among Low-Income US Adults in 4 Southern States
- PMID: 35977190
- PMCID: PMC8796874
- DOI: 10.1001/jamahealthforum.2021.2007
COVID-19-Related Insurance Coverage Changes and Disparities in Access to Care Among Low-Income US Adults in 4 Southern States
Abstract
Importance: It is unclear how the COVID-19 pandemic and its associated economic downturn have affected insurance coverage and disparities in access to health care among low-income families and people of color in states that have and have not expanded Medicaid.
Objective: To determine changes in insurance coverage and disparities in access to health care among low-income families and people of color across 4 Southern states and by Medicaid expansion status.
Design setting and participants: This random-digit dialing telephone survey study of US citizens ages 19 to 64 years with a family income less than 138% of the federal poverty line in in 4 states (Arkansas, Kentucky, Louisiana, and Texas) was conducted from October to December 2020. Using a difference-in-differences design, we estimated changes in outcomes by Medicaid expansion status overall and by race and ethnicity in 2020 (n = 1804) compared with 2018 to 2019 (n = 5710). We also explored barriers to health care and use of telehealth by race and ethnicity. Data analysis was conducted from January 2021 to March 2021.
Exposures: COVID-19 pandemic and prior Medicaid expansion status.
Main outcomes and measures: Primary outcome was the uninsured rate and secondary outcomes were financial and nonfinancial barriers to health care access.
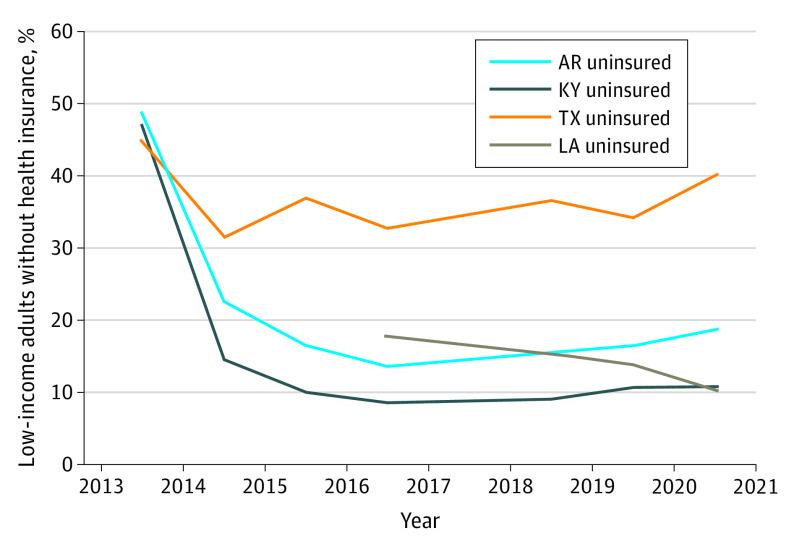
Results: Of 7514 respondents (11% response rate; 3889 White non-Latinx [51.8%], 1881 Black non-Latinx [25.0%], and 1156 Latinx individuals [15.4%]; 4161 women [55.4%]), 5815 (77.4%) were in the states with previous expansion and 1699 (22.6%) were in Texas (nonexpansion state). Respondents in the expansion states were older, more likely White, and less likely to have attended college compared with respondents in Texas. Uninsurance rate in 2020 rose by 7.4 percentage points in Texas (95% CI, 2.2-12.6; P = .01) and 2.5 percentage points in expansion states (95% CI, -1.9 to 7.0; P = .27), with a difference-in-differences estimate for Medicaid expansion of -4.9% (95% CI, -11.3 to 1.6; P = .14). Among Black and Latinx individuals, Medicaid expansion was associated with protection against a rise in the uninsured rate (difference-in-differences, -9.5%; 95% CI, -19.0 to -0.1; P = .048). Measures of access, including having a personal physician and regular care for chronic conditions, worsened significantly in 2020 in all 4 states, with no significant difference by Medicaid expansion status.
Conclusions and relevance: In this survey of US adults, uninsured rates increased among low-income adults in 4 Southern states during the COVID-19 pandemic, but Medicaid expansion states, that association was diminished among Black and Latinx individuals. Nonfinancial barriers to care because of the pandemic were common in all states.
Copyright 2021 Figueroa JF et al. JAMA Health Forum.
Conflict of interest statement
Conflict of Interest Disclosures: Dr Figueroa reported grants from the Commonwealth Fund and Robert Wood Johnson Foundation during the conduct of the study as well as grants from the Commonwealth Fund, Robert Wood Johnson Foundation, and Harvard Center for AIDS Research outside the submitted work. Drs Orav and Epstein reported grants from the Commonwealth Fund during the conduct of the study. Dr Sommers reported grants from the National Institute on Minority Health and Health Disparities, Robert Wood Johnson Foundation Policies for Action Program, and Commonwealth Fund during the conduct of the study as well as grants from Baylor Scott & White; personal fees from Health Services Research, Massachusetts Medical Society, Urban Institute, AcademyHealth, American Economics Journal, and the Illinois Department of Healthcare and Family Services; and service in the US Department of Health and Human Services. No other disclosures were reported.
Figures
Comment in
- doi: 10.1001/jamahealthforum.2021.2000
References
-
- Gangopadhyaya A, Karpman M, Aarons J. As the COVID-19 recession extended into the summer of 2020, more than 3 million adults lost employer-sponsored health insurance coverage and 2 million became uninsured. Accessed May 20, 2021. https://www.urban.org/sites/default/files/publication/102852/as-the-covi...
-
- McIntyre A, Brault MW, Sommers BD. Measuring coverage rates in a pandemic: policy and research challenges. JAMA Health Forum. 2020;1(10):e201278. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
