

Association Between Self-reported Health-Related Social Needs and Acute Care Utilization Among Older Adults Enrolled in Medicare Advantage
- PMID: 35977222
- PMCID: PMC9270697
- DOI: 10.1001/jamahealthforum.2022.1874
Association Between Self-reported Health-Related Social Needs and Acute Care Utilization Among Older Adults Enrolled in Medicare Advantage
Abstract
Importance: There is increased focus on identifying and addressing health-related social needs (HRSNs). Understanding how different HRSNs relate to different health outcomes can inform targeted, evidence-based policies, investments, and innovations to address HRSNs.
Objective: To examine the association between self-reported HRSNs and acute care utilization among older adults enrolled in Medicare Advantage.
Design setting and participants: This cross-sectional study used data from a large, national survey of Medicare Advantage beneficiaries to identify the presence of HRSNs. Survey data were linked to medical claims, and regression models were used to estimate the association between HRSNs and rates of acute care utilization from January 1, 2019, through December 31, 2019.
Exposures: Self-reported HRSNs, including food insecurity, financial strain, loneliness, unreliable transportation, utility insecurity, housing insecurity, and poor housing quality.
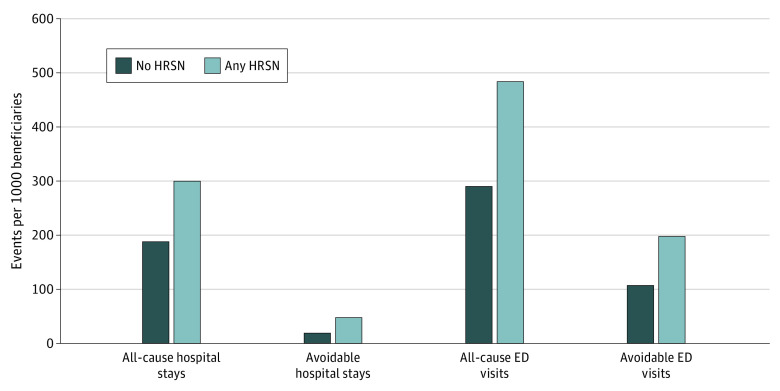
Main outcomes and measures: All-cause hospital stays (inpatient admissions and observation stays), avoidable hospital stays, all-cause emergency department (ED) visits, avoidable ED visits, and 30-day readmissions.
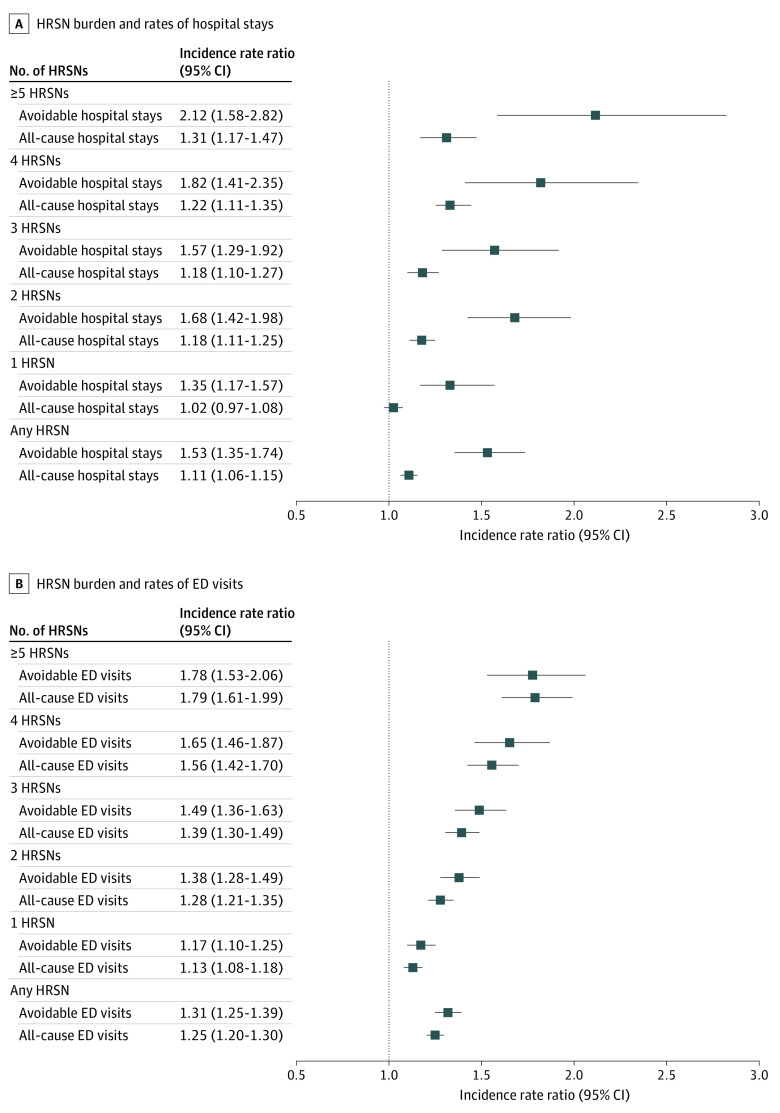
Results: Among a final study population of 56 155 Medicare Advantage beneficiaries (mean [SD] age, 74.0 [5.8] years; 32 779 [58.4%] women; 44 278 [78.8%] White; and 7634 [13.6%] dual eligible for Medicaid), 27 676 (49.3%) reported 1 or more HRSNs. Health-related social needs were associated with statistically significantly higher rates of all utilization measures, with the largest association observed for avoidable hospital stays (incident rate ratio for any HRSN, 1.53; 95% CI, 1.35-1.74; P < .001). Compared with beneficiaries without HRSNs, beneficiaries with an HRSN had a 53.3% higher rate of avoidable hospitalization (incident rate ratio, 1.53; 95% CI, 1.35-1.74; P < .001). Financial strain and unreliable transportation were each independently associated with increased rates of hospital stays (marginal effects of 26.5 [95% CI, 14.2-38.9] and 51.2 [95% CI, 30.7-71.8] hospital stays per 1000 beneficiaries, respectively). All HRSNs, except for utility insecurity, were independently associated with increased rates of ED visits. Unreliable transportation had the largest association with increased hospital stays and ED visits, with marginal effects of 51.2 (95% CI, 30.7-71.8) and 95.5 (95% CI, 65.3-125.8) ED visits per 1000 beneficiaries, respectively. Only unreliable transportation and financial strain were associated with increased rates of 30-day readmissions, with marginal effects of 3.3% (95% CI, 2.0%-4.0%) and 0.4% (95% CI, 0.2%-0.6%), respectively.
Conclusions and relevance: In this cross-sectional study of older adults enrolled in Medicare Advantage, self-reported HRSNs were common and associated with statistically significantly increased rates of acute care utilization, with variation in which HRSNs were associated with different utilization measures. These findings provide evidence of the unique association between certain HRSNs and different types of acute care utilization, which could help refine the development and targeting of efforts to address HRSNs.
Copyright 2022 Canterberry M et al. JAMA Health Forum.
Conflict of interest statement
Conflict of Interest Disclosures: Dr Figueroa reported personal fees from Humana during the conduct of the study, as well as grants from the Commonwealth Fund, the Robert Wood Johnson Foundation, the National Institute of Aging, and the Episcopal Health Foundation outside the submitted work. Dr Hagan, Ms Franklin, and Dr Renda reported equity holdings with Humana. Mr Gondi reported prior employment with Humana and the Commonwealth Care Alliance. Dr Shrank reported equity holdings with Humana and serving as a director at GetWellNetwork outside the submitted work. Dr Powers reported equity holdings with Humana and prior employment with Anthem and Fidelity Investments. No other disclosures were reported.
Figures
References
-
- National Academies of Sciences, Engineering, and Medicine . Integrating Social Care Into the Delivery of Health Care: Moving Upstream to Improve the Nation’s Health. The National Academies Press; 2019. - PubMed
-
- Engelberg Anderson JK, Jain P, Wade AJ, Morris AM, Slaboda JC, Norman GJ. Indicators of potential health-related social needs and the association with perceived health and well-being outcomes among community-dwelling Medicare beneficiaries. Qual Life Res. 2020;29(6):1685-1696. doi: 10.1007/s11136-019-02410-7 - DOI - PubMed
