

Factors Associated With Disparities in Hospital Readmission Rates Among US Adults Dually Eligible for Medicare and Medicaid
- PMID: 35977231
- PMCID: PMC8903116
- DOI: 10.1001/jamahealthforum.2021.4611
Factors Associated With Disparities in Hospital Readmission Rates Among US Adults Dually Eligible for Medicare and Medicaid
Abstract
Importance: Low-income older adults who are dually eligible (DE) for Medicare and Medicaid often experience worse outcomes following hospitalization. Among other federal policies aimed at improving health for DE patients, Medicare has recently begun reporting disparities in within-hospital readmissions. The degree to which disparities for DE patients are owing to differences in community-level factors or, conversely, are amenable to hospital quality improvement, remains heavily debated.
Objective: To examine the extent to which within-hospital disparities in 30-day readmission rates for DE patients are ameliorated by state- and community-level factors.
Design setting and participants: In this retrospective cohort study, Centers for Medicare & Medicaid Services (CMS) Disparity Methods were used to calculate within-hospital disparities in 30-day risk-adjusted readmission rates for DE vs non-DE patients in US hospitals participating in Medicare. All analyses were performed in February and March 2019. The study included Medicare patients (aged ≥65 years) hospitalized for acute myocardial infarction (AMI), heart failure (HF), or pneumonia in 2014 to 2017.
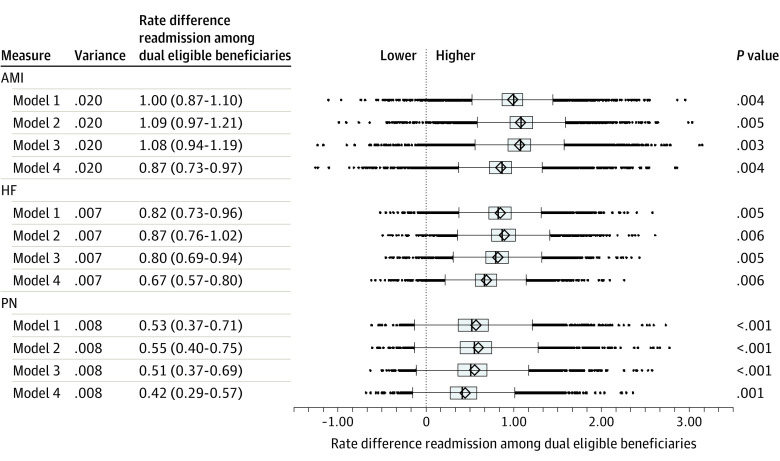
Main outcomes and measures: Within-hospital disparities, as measured by the rate difference (RD) in 30-day readmission between DE vs non-DE patients following admission for AMI, HF, or pneumonia; variance across hospitals; and correlation of hospital RDs with and without adjustment for state Medicaid eligibility policies and community-level factors.
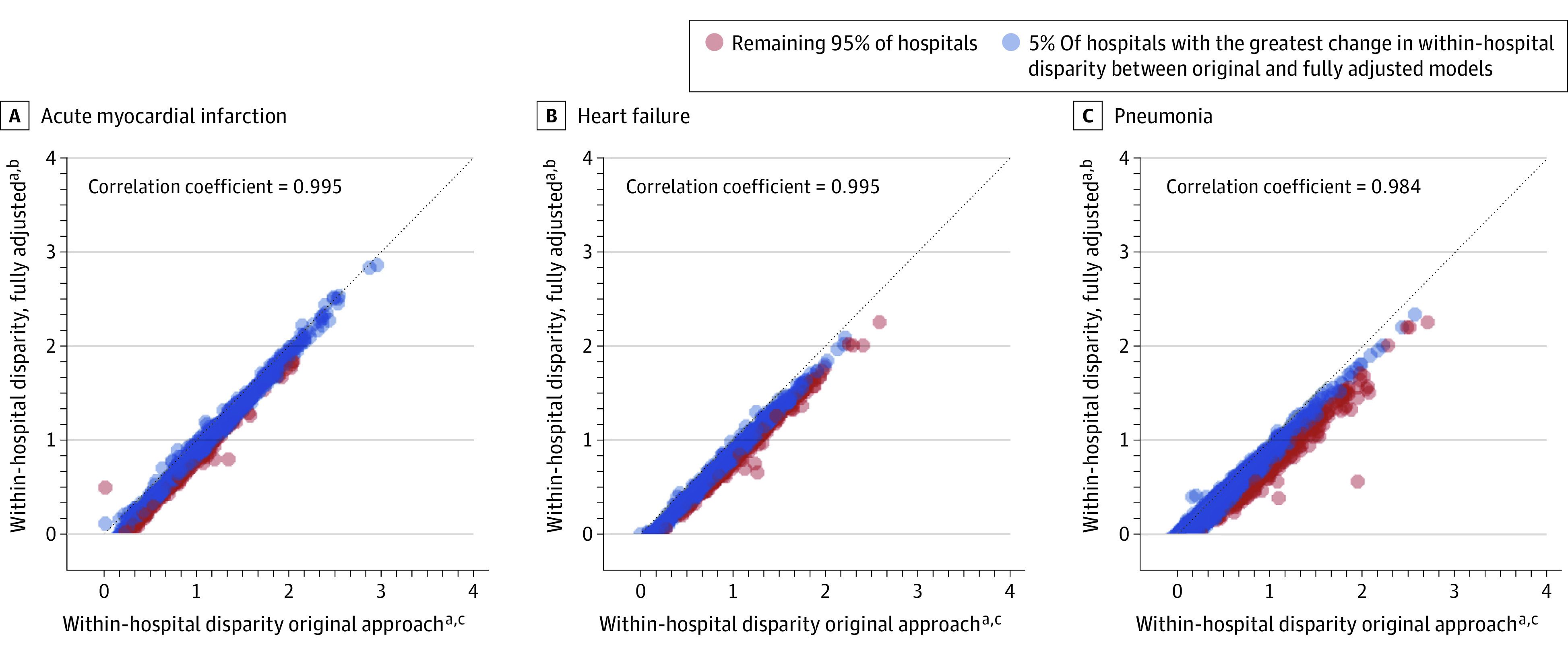
Results: The final sample included 475 444 patients admitted for AMI, 898 395 for HF, and 1 214 282 for pneumonia, of whom 13.2%, 17.4%, and 23.0% were DE patients, respectively. Dually eligible patients had higher 30-day readmission rates relative to non-DE patients (RD >0) in 99.0% (AMI), 99.4% (HF), and 97.5% (pneumonia) of US hospitals. Across hospitals, the mean (IQR) RD between DE vs non-DE was 1.00% (0.87%-1.10%) for AMI, 0.82% (0.73%-0.96%) for HF, and 0.53% (0.37%-0.71%) for pneumonia. The mean (IQR) RD after adjustment for community-level factors was 0.87% (0.73%-0.97%) for AMI, 0.67% (0.57%-0.80%) for HF, and 0.42% (0.29%-0.57%) for pneumonia. Relative hospital rankings of corresponding within-hospital disparities before and after community-level adjustment were highly correlated (Pearson coefficient, 0.98).
Conclusions and relevance: In this cohort study, within-hospital disparities in 30-day readmission for DE patients were modestly associated with differences in state Medicaid policies and community-level factors. This suggests that remaining variation in these disparities should be the focus of hospital efforts to improve the quality of care transitions at discharge for DE patients in efforts to advance equity.
Copyright 2022 Silvestri D et al. JAMA Health Forum.
Conflict of interest statement
Conflict of Interest Disclosures: Dr Silvestri is currently employed by NYC Health and Hospitals but completed this work at Yale University while supported in part through CTSA Grant Number TL1 TR001864 from the National Center for Advancing Translational Science (NCATS), a component of the National Institutes of Health (NIH). Drs Peltz, Lloren, Zhou S, Zhou G, Farietta, Herrin, Lin, and Bernheim, Ms Charania, and Mr Goutos completed this work while working as employees or consultants at Yale New Haven Health Services Corporation/Center for Outcomes Research & Evaluation (YNHHSC/CORE). This work was supported by the Centers for Medicare & Medicaid Services (CMS) under contract HHSM-500-2013-13018I/HHSM-500-T0001.
Figures
Similar articles
-
Association of Changing Hospital Readmission Rates With Mortality Rates After Hospital Discharge.JAMA. 2017 Jul 18;318(3):270-278. doi: 10.1001/jama.2017.8444. JAMA. 2017. PMID: 28719692 Free PMC article.
-
Association of Frailty With 30-Day Outcomes for Acute Myocardial Infarction, Heart Failure, and Pneumonia Among Elderly Adults.JAMA Cardiol. 2019 Nov 1;4(11):1084-1091. doi: 10.1001/jamacardio.2019.3511. JAMA Cardiol. 2019. PMID: 31553402 Free PMC article.
-
Association Between Medicare Expenditures and Adverse Events for Patients With Acute Myocardial Infarction, Heart Failure, or Pneumonia in the United States.JAMA Netw Open. 2020 Apr 1;3(4):e202142. doi: 10.1001/jamanetworkopen.2020.2142. JAMA Netw Open. 2020. PMID: 32259263 Free PMC article.
-
A review of socioeconomic factors associated with acute myocardial infarction-related mortality and hospital readmissions.Hosp Pract (1995). 2022 Feb;50(1):1-8. doi: 10.1080/21548331.2021.2022357. Epub 2022 Jan 6. Hosp Pract (1995). 2022. PMID: 34933647 Review.
-
Rural-urban disparities in mortality of patients with acute myocardial infarction and heart failure: a systematic review and meta-analysis.Eur J Prev Cardiol. 2025 Mar 18;32(4):327-335. doi: 10.1093/eurjpc/zwae351. Eur J Prev Cardiol. 2025. PMID: 39470401
Cited by
-
The Relative Importance of Hospital Discharge and Patient Composition in Changing Post-Acute Care Utilization and Outcomes Among Medicare Beneficiaries.Health Serv Insights. 2023 Apr 14;16:11786329231166522. doi: 10.1177/11786329231166522. eCollection 2023. Health Serv Insights. 2023. PMID: 37077324 Free PMC article.
-
Predicting quality measure completion among 14 million low-income patients enrolled in medicaid.NPJ Digit Med. 2025 Jul 2;8(1):393. doi: 10.1038/s41746-025-01797-7. NPJ Digit Med. 2025. PMID: 40604098 Free PMC article.
-
Quality of care for dual eligible beneficiaries in the oncology care model.Cancer Med. 2024 Jul;13(14):e70009. doi: 10.1002/cam4.70009. Cancer Med. 2024. PMID: 39030893 Free PMC article.
-
Heart Failure in Black Populations: Epidemiology, Pathophysiology, and Treatment Disparities.J Racial Ethn Health Disparities. 2025 Mar 7. doi: 10.1007/s40615-025-02371-3. Online ahead of print. J Racial Ethn Health Disparities. 2025. PMID: 40053215 Review.
-
Measuring Equity in Readmission as a Distinct Assessment of Hospital Performance.JAMA. 2024 Jan 9;331(2):111-123. doi: 10.1001/jama.2023.24874. JAMA. 2024. PMID: 38193960 Free PMC article.
References
-
- Centers for Medicare and Medicaid Services (CMS) . Medicare program; hospital inpatient prospective payment systems for acute care hospitals and the long-term care hospital prospective payment system and proposed policy changes and fiscal year 2022 rates; quality programs and Medicare promoting interoperability program requirements for eligible hospitals and critical access hospitals; proposed changes to Medicaid provider enrollment; and proposed changes to the Medicare Shared Savings Program. Federal Registrar. 862021:25070-25790; 2021.
-
- Medicaid and CHIP Payment and Access Commission (MACPAC) . MACStats: Meidcaid and CHIP Data Book. Section 4, Exhibit 37: Medicaid Income Eligibility Levels as a Percentage of the Federal Poverty Level for Individuals Age 65 and Older and Persons with Disabilities by State. 2017. Accessed June 6, 2021. https://medpac.gov/docs/default-source/payment-basics/medpac_payment_bas...
-
- Centers for Medicare and Medicaid Services (CMS) . Confidential Reporting Overview: Disparity Methods. Accessed March 4, 2019. https://www.qualitynet.org/dcs/ContentServer?c=Page&pagename=QnetPublic/...
-
- Centers for Medicare and Medicaid Services (CMS) . Medicare program; hospital inpatient prospective payment systems for acute care hospitals and the longterm care hospital prospective payment system and policy changes and fiscal year 2018 rates; quality reporting requirements for specific providers. Federal Registrar. 2017;822017:38403-38409. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
