

Physician Practice Pattern Variations in Common Clinical Scenarios Within 5 US Metropolitan Areas
- PMID: 35977237
- PMCID: PMC8903123
- DOI: 10.1001/jamahealthforum.2021.4698
Physician Practice Pattern Variations in Common Clinical Scenarios Within 5 US Metropolitan Areas
Abstract
Importance: While variations in quality of care have been described between US regions, physician-level practice pattern variations within regions remain poorly understood, notably among specialists.
Objective: To examine within-area physician-level variations in decision-making in common clinical scenarios where guidelines specifying appropriateness or quality of care exist.
Design setting and participants: This cross-sectional study used 2016 through 2019 data from a large nationwide network of commercial insurers, provided by Health Intelligence Company, LLC, within 5 metropolitan statistical areas (MSAs). Physician-level variations in appropriateness and quality of care were measured using 14 common clinical scenarios involving 7 specialties. The measures were constructed using public quality measure definitions, clinical guidelines, and appropriateness criteria from the clinical literature. Physician performance was calculated using a multilevel model adjusted for patient age, sex, risk score, and socioeconomic status with physician random effects. Measure reliability for each physician was calculated using the signal-to-noise approach. Within-MSA variation was calculated between physician quintiles adjusted for patient attributes, with the first quintile denoting highest quality or appropriateness and the fifth quintile reflecting the opposite. Data were analyzed March through October 2021.
Main outcomes and measures: Fourteen measures of quality or appropriateness of care, with 2 measures each in the domains of cardiology, endocrinology, gastroenterology, pulmonology, obstetrics, orthopedics, and neurosurgery.
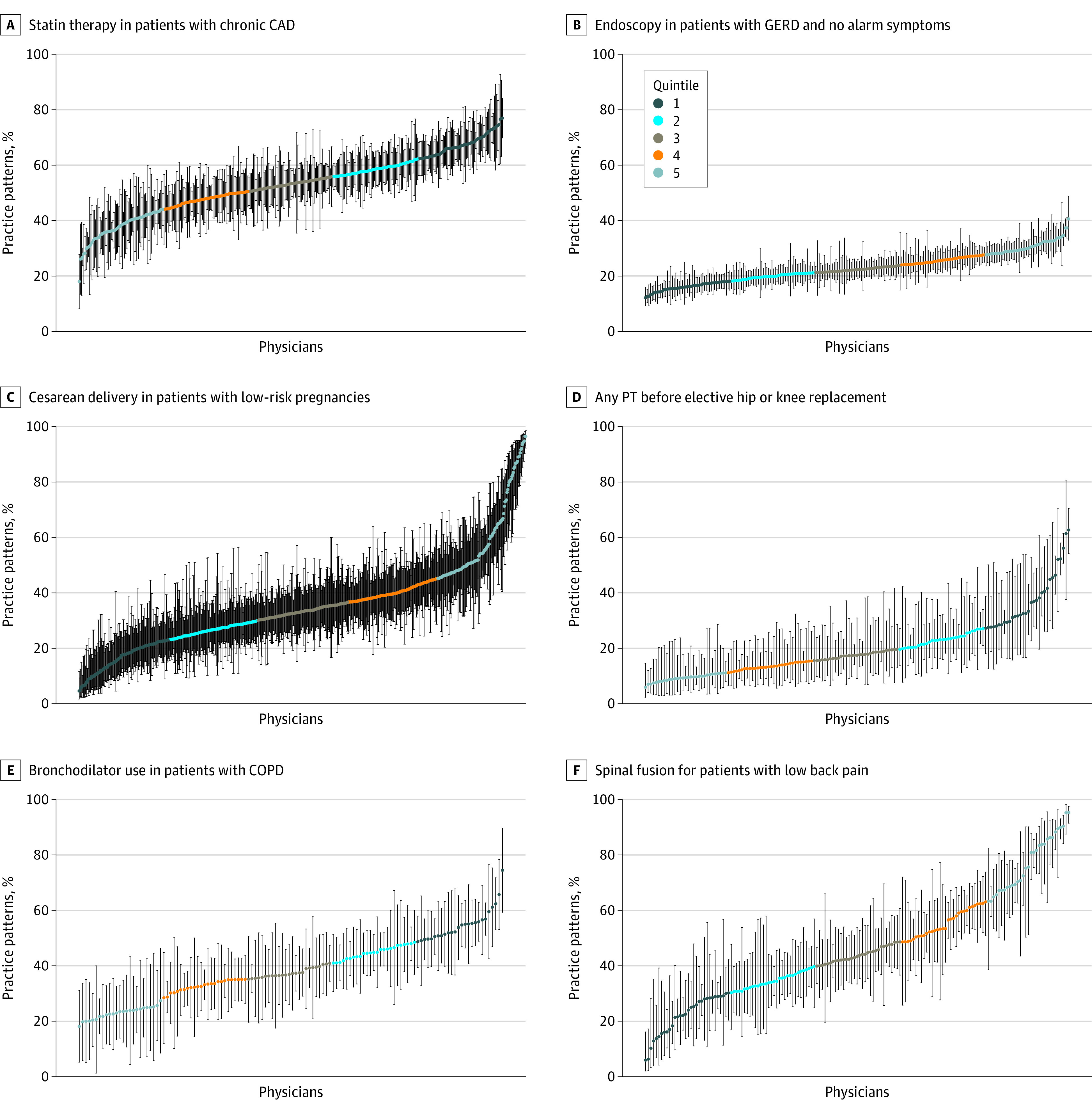
Results: A total of 8788 physicians were included across the 5 MSAs, and about 2.5 million unique patient-physician pairs were included in the measures. Within the 5 MSAs, on average, patients in the measures were 34.7 to 40.7 years old, 49.1% to 52.3% female, had a mean risk score of 0.8 to 1.0, and more likely to have an employer-sponsored insurance plan that was either self-insured or fully insured (59.8% to 97.6%). Within MSAs, physician-level variations were qualitatively similar across measures. For example, statin therapy in patients with coronary artery disease ranged from 54.3% to 70.9% in the first quintile of cardiologists to 30.5% to 42.6% in the fifth quintile. Upper endoscopy in patients with gastroesophageal reflux disease without alarm symptoms spanned 14.6% to 16.9% in the first quintile of gastroenterologists to 28.2% to 33.8% in the fifth quintile. Among patients with new knee or hip osteoarthritis, 2.1% to 3.4% received arthroscopy in the first quintile of orthopedic surgeons, whereas 25.5% to 30.7% did in the fifth quintile. Appropriate prenatal screening among pregnant patients ranged from 82.6% to 93.6% in the first quintile of obstetricians to 30.9% to 65.7% in the fifth quintile. Within MSAs, adjusted differences between quintiles approximated unadjusted differences. Measure reliability, which can reflect consistency and reproducibility, exceeded 70.0% across nearly all measures in all MSAs.
Conclusions and relevance: In this cross-sectional study of 5 US metropolitan areas, sizeable physician-level practice variations were found across common clinical scenarios and specialties. Understanding the sources of these variations may inform efforts to improve the value of care.
Copyright 2022 Song Z et al. JAMA Health Forum.
Conflict of interest statement
Conflict of Interest Disclosures: Dr Song reported personal fees from the Research Triangle Institute for work on Medicare risk adjustment; from Google Ventures, VBID Health LLC, and the International Foundation of Employee Benefit Plans for academic lectures outside of this work; and for providing consultation in legal cases. Dr Vaduganathan reported grants from Amgen, AstraZeneca, Boehringer Ingelheim, and Roche Diagnostics, as well as personal fees from American Regent, Baxter, Bayer AG, Boehringer Ingelheim, Cytokinetics, Relypsa, Novartis, Roche Diagnostics, Lexicon Pharmaceuticals, and Galmed outside the submitted work. Dr Bloom reported grants from the American College of Gastroenterology, the American Association for the Study of Liver Diseases, and Vedanta Biosciences outside the submitted work, as well as consulting fees from Synlogic Inc. Dr Resnick reported pending patents (P14431.1 and P14432.1) through Embold Health. No other disclosures were reported.
Figures
Comment in
-
Socioeconomic Factors, Urological Epidemiology and Practice Patterns.J Urol. 2022 Oct;208(4):921-922. doi: 10.1097/JU.0000000000002850. Epub 2022 Aug 1. J Urol. 2022. PMID: 35914314 No abstract available.
Similar articles
-
Association of Clinical Characteristics With Variation in Emergency Physician Preferences for Patients.JAMA Netw Open. 2020 Jan 3;3(1):e1919607. doi: 10.1001/jamanetworkopen.2019.19607. JAMA Netw Open. 2020. PMID: 31968113 Free PMC article.
-
Association Between Patient Social Risk and Physician Performance Scores in the First Year of the Merit-based Incentive Payment System.JAMA. 2020 Sep 8;324(10):975-983. doi: 10.1001/jama.2020.13129. JAMA. 2020. PMID: 32897345 Free PMC article.
-
Profiling care provided by different groups of physicians: effects of patient case-mix (bias) and physician-level clustering on quality assessment results.Ann Intern Med. 2002 Jan 15;136(2):111-21. doi: 10.7326/0003-4819-136-2-200201150-00008. Ann Intern Med. 2002. PMID: 11790062
-
Using Consistently Low Performance to Identify Low-Quality Physician Groups.JAMA Netw Open. 2021 Jul 1;4(7):e2117954. doi: 10.1001/jamanetworkopen.2021.17954. JAMA Netw Open. 2021. PMID: 34319356 Free PMC article.
-
Establishing patient-specific criteria for selecting the optimal upper extremity vascular access procedure.J Vasc Surg. 2017 Apr;65(4):1089-1103.e1. doi: 10.1016/j.jvs.2016.10.099. Epub 2017 Feb 17. J Vasc Surg. 2017. PMID: 28222990 Free PMC article. Review.
Cited by
-
Machine learning for healthcare that matters: Reorienting from technical novelty to equitable impact.PLOS Digit Health. 2024 Apr 15;3(4):e0000474. doi: 10.1371/journal.pdig.0000474. eCollection 2024 Apr. PLOS Digit Health. 2024. PMID: 38620047 Free PMC article.
-
Accounting for Healthcare Structures When Measuring Variation in Care.Anesthesiology. 2025 May 1;142(5):793-805. doi: 10.1097/ALN.0000000000005395. Epub 2025 Apr 8. Anesthesiology. 2025. PMID: 40197451 Review.
-
Variation in Emergency Department Physician Admitting Practices and Subsequent Mortality.JAMA Intern Med. 2025 Feb 1;185(2):153-160. doi: 10.1001/jamainternmed.2024.6925. JAMA Intern Med. 2025. PMID: 39714798
-
Small bowel obstruction outcomes according to compliance with the World Society of Emergency Surgery Bologna guidelines.Br J Surg. 2025 Mar 28;112(4):znaf080. doi: 10.1093/bjs/znaf080. Br J Surg. 2025. PMID: 40246692 Free PMC article.
-
Health Disparity Clusters of Off Label Prescriptions for Glucagon-Like Peptide 1 Receptor Agonists.Am J Med Open. 2025 Apr 4;13:100100. doi: 10.1016/j.ajmo.2025.100100. eCollection 2025 Jun. Am J Med Open. 2025. PMID: 40496649 Free PMC article.
References
-
- Newhouse JP, Garber AM, Graham RP, McCoy MA, Mancher M, Kibria A, eds. Variation in Health Care Spending: Target Decision Making, Not Geography. The National Academies Press; 2013. - PubMed
