

Spending by the Centers for Medicare & Medicaid Services Before and After Confirmation of Benefit for Drugs Granted US Food and Drug Administration Accelerated Approval, 2012 to 2017
- PMID: 35977252
- PMCID: PMC9142876
- DOI: 10.1001/jamahealthforum.2022.1158
Spending by the Centers for Medicare & Medicaid Services Before and After Confirmation of Benefit for Drugs Granted US Food and Drug Administration Accelerated Approval, 2012 to 2017
Abstract
Importance: Accelerated approval by the US Food and Drug Administration (FDA) grants market authorization for drugs based on clinical trials using surrogate end points likely to anticipate a clinical benefit. The FDA requires postapproval trials to confirm benefit, after which the accelerated approval is converted to a standard approval or is withdrawn. However, trials frequently fail to assess clinical benefit, and expenditure for these drugs may be substantial.
Objective: To evaluate spending by the Centers for Medicare & Medicaid Services (CMS) on drugs granted FDA accelerated approval before and after confirmation of benefit.
Design and setting: This was a cross-sectional study of CMS spending on drugs granted FDA accelerated approval for original indications from 2012 to 2017, with follow-up through 2020. Using data from the Drugs@FDA database and a validated methodology, the characteristics of new drugs granted FDA accelerated approval were identified and analyzed, including indication area, type of drug, type of confirmatory trial end point, orphan designation, number of supplemental indications, and conversion status.
Main outcomes and measures: Overall and annualized spending by Medicare Parts B and D and Medicaid from 2012 to 2020, before and after conversion to standard approval. Analyses were conducted from June 30, 2021, to March 21, 2022.
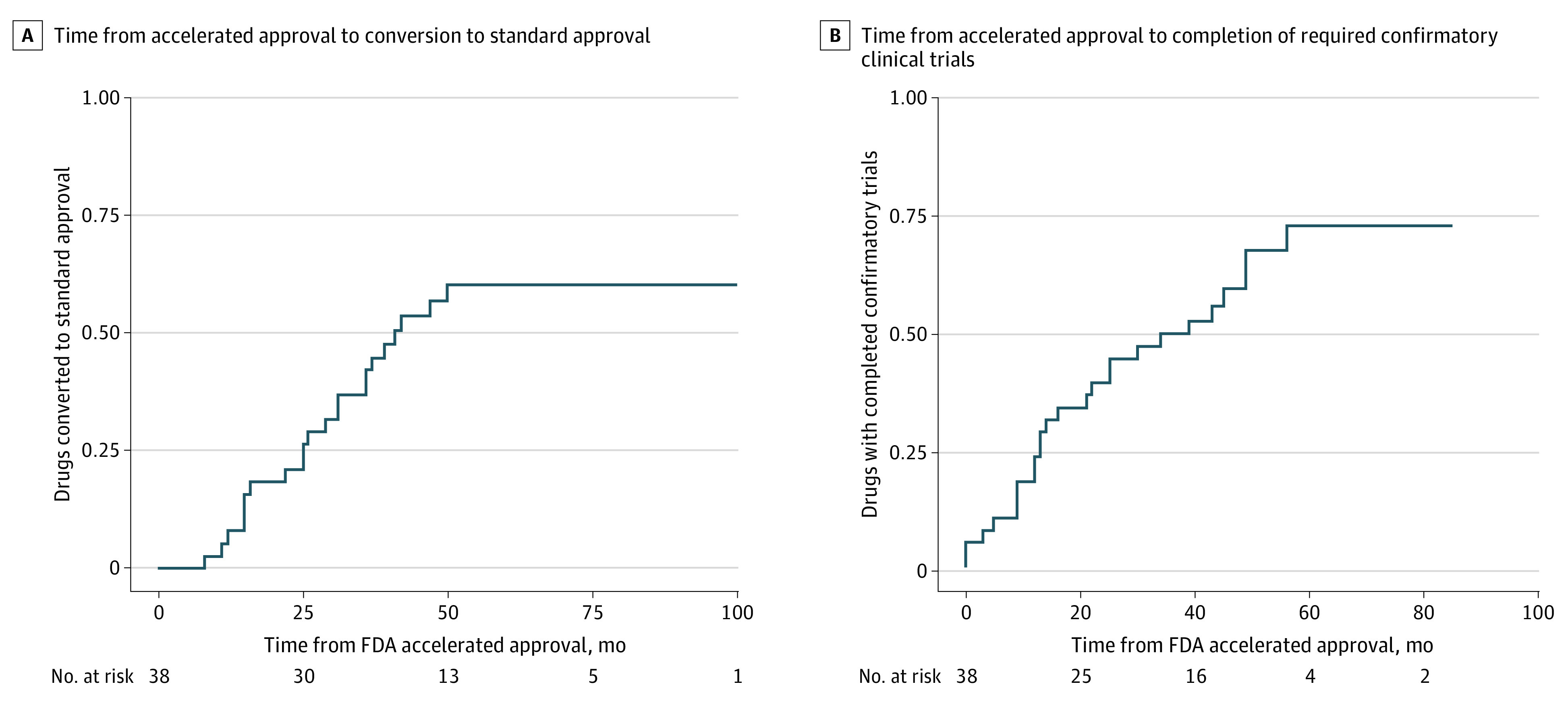
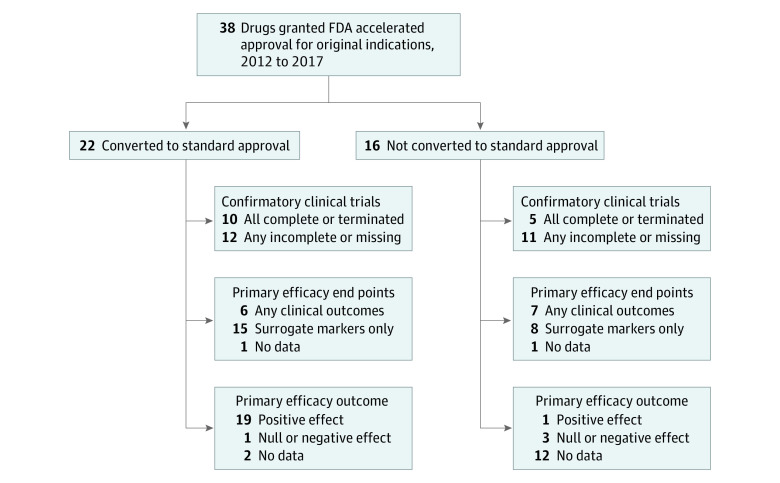
Results: From 2012 to 2017, the FDA granted accelerated approval to 38 drugs for 42 original indications. Through 2020, CMS spending for these drugs was $67.9 billion (median [IQR], $329.3 million [$54.4 million-$1.6 billion]). For 22 drugs (58%) that were converted to standard approval on the basis of clinical trial results, annualized spending increased substantially after conversion ($35.0 million vs $199.0 million), and spending after conversion accounted for $51.0 billion (75%) of overall spending. However, only 6 conversions (27%) of the 22 were supported by confirmatory trials evaluating clinical outcomes as primary end points. Drugs evaluated using surrogate end points accounted for $40.3 billion (59%) of CMS spending.
Conclusions and relevance: The findings of this cross-sectional study indicate that most of the drugs granted FDA accelerated approval for original indications from 2012 to 2017 lacked confirmatory trials evaluating clinical outcomes to support conversion to standard approval. Automatic coverage mandates produced substantial CMS spending for drugs with unproven clinical benefits.
Copyright 2022 Skydel JJ et al. JAMA Health Forum.
Conflict of interest statement
Conflict of Interest Disclosures: Dr Skydel is a member of the US Food and Drug Administration (FDA) Task Force for Doctors for America, outside the submitted work. Mr Egilman reported grants from Arnold Ventures and research support through Yale University from the Laura and John Arnold Foundation for the Collaboration for Research Integrity and Transparency and from the FDA for the Yale−Mayo Clinic Center for Excellence in Regulatory Science and Innovation program (No. U01FD005938), all outside the submitted work. Dr Wallach reported support from the National Institute on Alcohol Abuse and Alcoholism of the National Institutes of Health (NIH; No. K01AA028258), the FDA, and through Yale University from Johnson & Johnson to develop methods of clinical data sharing, all outside the submitted work. Dr Ramachandran reported serving on the boards of Universities Allied for Essential Medicines North America and the American Medical Student Association Foundation as an uncompensated member and serving as a chairperson for the FDA Task Force for Doctors for America, outside the submitted work. Dr Ross reported research support through Yale University from Johnson & Johnson to develop methods of clinical trial data sharing and from the Medical Device Innovation Consortium and grants from the FDA for the Yale–Mayo Clinic Center for Excellence in Regulatory Science and Innovation program (No. U01FD005938), the AHRQ (No. R01HS022882), the NIH National Heart, Lung and Blood Institute (Nos. R01HS025164; R01HL144644), and from the Laura and John Arnold Foundation, all outside of the submitted work. In addition, Dr Ross reported being an expert witness at the request of Relator’s attorneys, the Greene Law Firm, in a qui tam suit alleging violations of the False Claims Act and Anti-Kickback Statute against Biogen. No other disclosures were reported.
Figures
Similar articles
-
Improving Food and Drug Administration-Centers for Medicare and Medicaid Services Coordination for Drugs Granted Accelerated Approval.Milbank Q. 2023 Dec;101(4):1047-1075. doi: 10.1111/1468-0009.12670. Epub 2023 Aug 29. Milbank Q. 2023. PMID: 37644739 Free PMC article.
-
Recent Trends in Medicaid Spending and Use of Drugs With US Food and Drug Administration Accelerated Approval.JAMA Health Forum. 2021 Oct 8;2(10):e213177. doi: 10.1001/jamahealthforum.2021.3177. eCollection 2021 Oct. JAMA Health Forum. 2021. PMID: 35977163 Free PMC article.
-
Medicare Spending on Drugs With Accelerated Approval.Ann Intern Med. 2022 Jul;175(7):938-944. doi: 10.7326/M21-4442. Epub 2022 May 24. Ann Intern Med. 2022. PMID: 35605235
-
Assessment of the Clinical Benefit of Cancer Drugs Receiving Accelerated Approval.JAMA Intern Med. 2019 Jul 1;179(7):906-913. doi: 10.1001/jamainternmed.2019.0462. JAMA Intern Med. 2019. PMID: 31135808 Free PMC article. Review.
-
Accelerated approval of oncology products: the food and drug administration experience.J Natl Cancer Inst. 2011 Apr 20;103(8):636-44. doi: 10.1093/jnci/djr062. Epub 2011 Mar 21. J Natl Cancer Inst. 2011. PMID: 21422403 Review.
Cited by
-
Aducanumab, Accelerated Approvals & the Agency: Why the FDA Needs Structural Reform.J Law Med Ethics. 2023;51(4):900-919. doi: 10.1017/jme.2024.20. Epub 2024 Mar 13. J Law Med Ethics. 2023. PMID: 38477277 Free PMC article.
-
Added Therapeutic Benefit of Top-Selling Brand-name Drugs in Medicare.JAMA. 2023 Apr 18;329(15):1283-1289. doi: 10.1001/jama.2023.4034. JAMA. 2023. PMID: 37071095 Free PMC article.
-
Characterization of accelerated approval status, trial endpoints and results, and recommendations in guidelines for oncology drug treatments from the National Comprehensive Cancer Network: cross sectional study.BMJ Med. 2024 Apr 5;3(1):e000802. doi: 10.1136/bmjmed-2023-000802. eCollection 2024. BMJ Med. 2024. PMID: 38596814 Free PMC article.
-
Improving Food and Drug Administration-Centers for Medicare and Medicaid Services Coordination for Drugs Granted Accelerated Approval.Milbank Q. 2023 Dec;101(4):1047-1075. doi: 10.1111/1468-0009.12670. Epub 2023 Aug 29. Milbank Q. 2023. PMID: 37644739 Free PMC article.
-
The high costs of anticancer therapies in the USA: challenges, opportunities and progress.Nat Rev Clin Oncol. 2024 Dec;21(12):888-899. doi: 10.1038/s41571-024-00948-1. Epub 2024 Oct 4. Nat Rev Clin Oncol. 2024. PMID: 39367130 Free PMC article. Review.
References
-
- United States Food and Drug Administration . Accelerated Approval. Published online November 3, 2018. Accessed March 14, 2022. https://www.fda.gov/patients/fast-track-breakthrough-therapy-accelerated...
-
- United States Food and Drug Administration . Guidance for industry: expedited programs for serious conditions: drugs and biologics. May 2014. Accessed March 14, 2022. https://www.fda.gov/media/86377/download
-
- United States Food and Drug Administration . CDER drug and biologic accelerated approvals based on a surrogate endpoint. Published online January 27, 2022. Accessed March 14, 2022. https://www.fda.gov/media/151146/download
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
