

Evaluation of Federal Policy Changes to the Hospice Benefit and Use of Hospice for Persons With ADRD
- PMID: 35977261
- PMCID: PMC9077487
- DOI: 10.1001/jamahealthforum.2022.0900
Evaluation of Federal Policy Changes to the Hospice Benefit and Use of Hospice for Persons With ADRD
Abstract
Importance: Hospice is an important end-of-life service for patients with Alzheimer disease and related dementias (ADRD).
Objective: To determine whether hospice use among patients with ADRD changed in association with recent policies aimed at reducing hospice misuse and long hospice stays, an outcome that may have disproportionately affected patients with ADRD because of their lengthy end-of-life trajectories.
Design setting and participants: This observational cross-sectional study used Medicare hospice claims data from Medicare hospice episodes of care beginning between July 2008 and December 2019 among Medicare hospice beneficiaries 65 years or older at time of enrollment. Data analysis was conducted between September 2019 and June 2021.
Exposures: The 2014 Improving Medicare Post-Acute Care Transformation (IMPACT) Act, which systematized audits of hospices with a high proportion of long stays, and the 2016 2-tier payment system, which reduced daily reimbursement rates after 60 days.
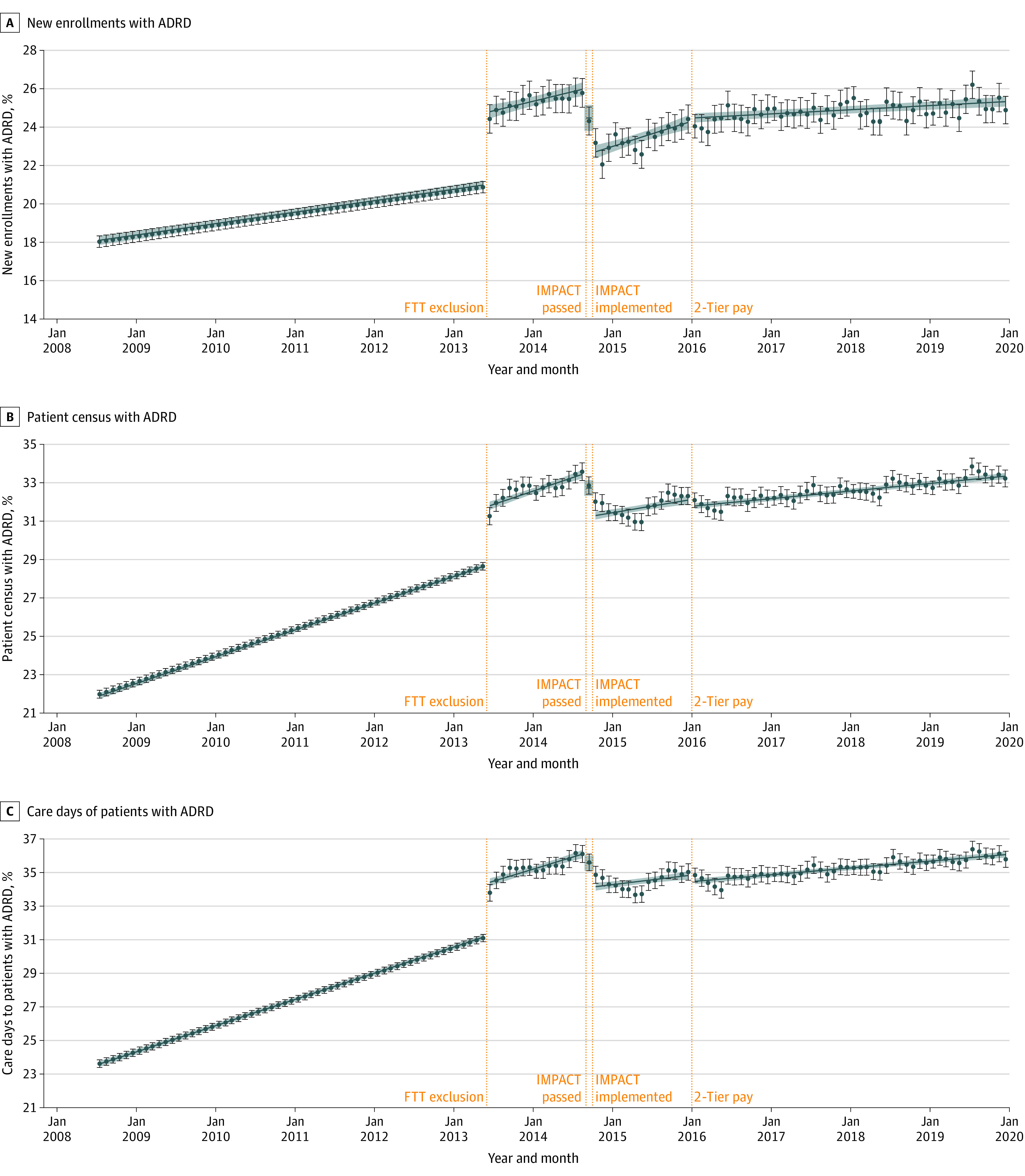
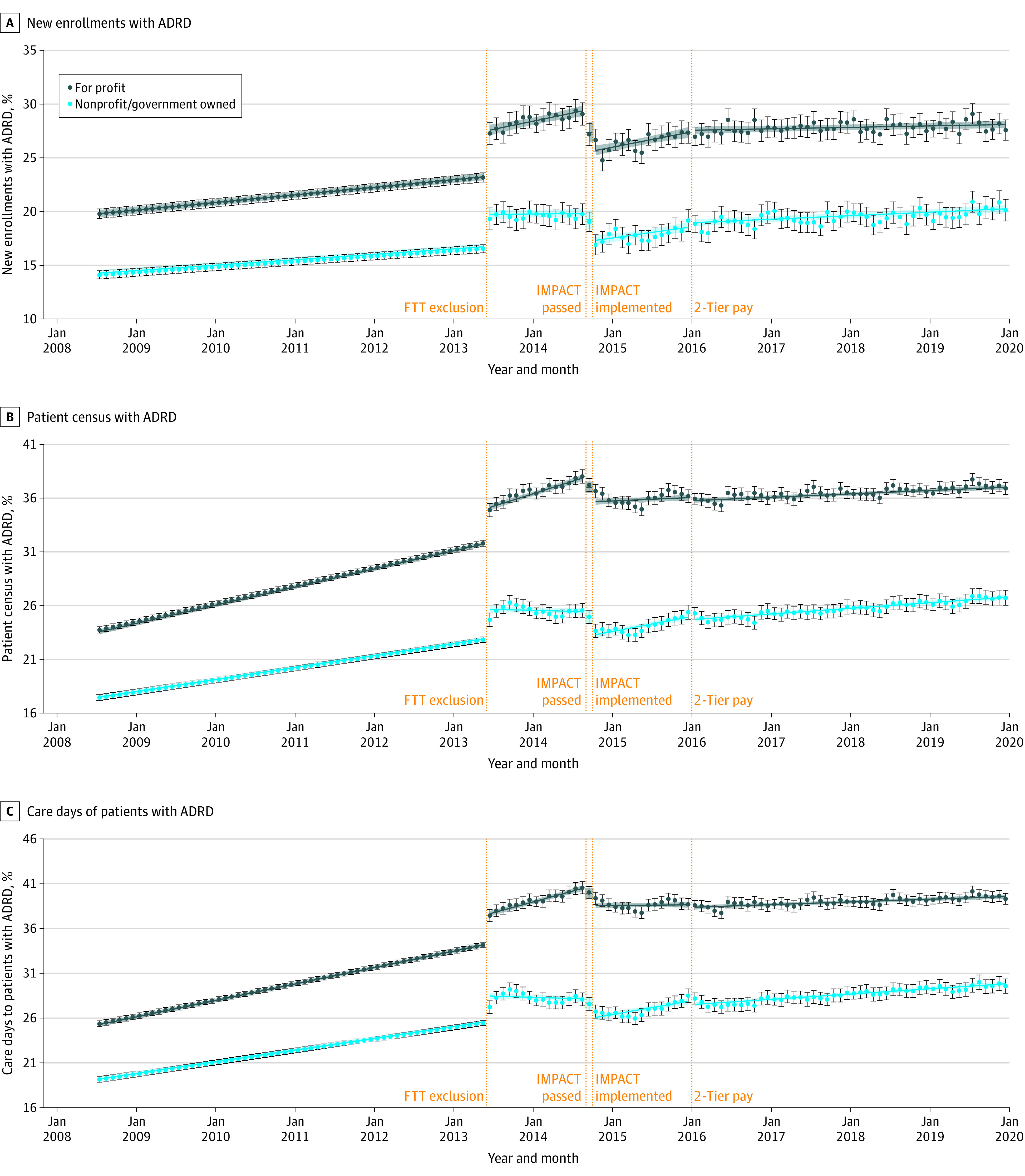
Main outcomes and measures: Monthly percentage of (1) new patient enrollees, (2) patient census, and (3) care days provided to patients with an ADRD code.
Results: The sample included 11 124 992 unique hospice episodes between 2008 and 2019; mean (SD) patient enrollment age ranged from 82.0 (8.2) years to 82.8 (8.7) years; the percentage of male patients ranged from 40.5% to 42.7%, and the percentage of Black, Hispanic, and White patients ranged from 7.7% to 8.2%, 1.5% to 2.0%, and 86.2% to 88.8%, respectively, across years. The percentage of new enrollees with an ADRD code dropped significantly during the months of IMPACT passage (-1.42 percentage points; 95% CI, -2.13 to -0.71) and implementation (-1.98 percentage points; 95% CI, -2.70 to -1.26) but rose again during the following months. While no significant changes were observed at the time of 2-tier payment implementation (0.15 percentage points; 95% CI, -0.21 to 0.51), the average rate of increase during the subsequent period was slower (0.01 percentage points per month; 95% CI, 0-0.02) than in earlier periods (0.05; 95% CI, 0.04-0.06 during the baseline period). Similar patterns were observed for the percentage of patient census and care days provided to patients with an ADRD code.
Conclusions and relevance: The results of this cross-sectional study of Medicare hospice claims data suggested that recent Medicare policies were associated with immediate and lasting reductions in the share of patients receiving hospice care with an ADRD code compared with expectations from preimplementation trends. Future research should examine mechanisms through which hospices enacted change and consequences for quality of care.
Copyright 2022 Gianattasio KZ et al. JAMA Health Forum.
Conflict of interest statement
Conflict of Interest Disclosures: Dr Gianattasio reported grants from National Institute of Aging (NIA; 5R03AG061499-02) during the conduct of the study. Dr Moghtaderi reported grants from the NIA during the conduct of the study. Dr Lupu reported grants from George Washington University during the conduct of the study and research support George Washington University outside the submitted work, as well as a patent for copyright with royalties from Oxford University Press. Dr Prather reported grants from the National Institutes of Health during the conduct of the study. Dr Power reported grants from NIA during the conduct of the study and personal fees from Biogen and grants from DC Health outside the submitted work.
Figures
References
-
- Institute of Medicine . Dying in America: Improving Quality and Honoring Individual Preferences near the End of Life. National Academies Press; 2015. - PubMed
-
- Volicer L, Hurley A. Hospice Care for Patients with Advanced Progressive Dementia. Springer Publishing Company, Inc; 1998.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
