

Rural Hospital Administrators' Beliefs About Safety, Financial Viability, and Community Need for Offering Obstetric Care
- PMID: 35977287
- PMCID: PMC8956977
- DOI: 10.1001/jamahealthforum.2022.0204
Rural Hospital Administrators' Beliefs About Safety, Financial Viability, and Community Need for Offering Obstetric Care
Abstract
Importance: Rural obstetric unit closures are associated with adverse maternal and infant health outcomes and are most common among low-birth volume facilities located in remote areas. Declining access to obstetric care is a concern in rural communities in the US.
Objective: To assess rural hospital administrators' beliefs about safety, financial viability, and community need for offering obstetric care.
Design setting and participants: Using the American Hospital Association Annual Survey to identify rural hospitals with obstetric units, we developed and conducted a national survey of a sample of rural hospitals that provided obstetric services in 2021. Obstetric unit managers or administrators at 292 rural hospitals providing obstetric services were surveyed from March to August 2021.
Exposures: Local factors, clinical safety, workforce, and financial considerations for obstetric services at participating hospitals.
Main outcomes and measures: Hospital-level decisions on maintaining obstetric care.
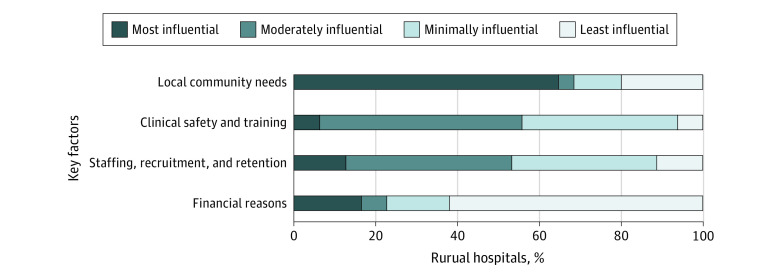
Results: Of the 93 total responding hospitals (32% response rate), 33 (35.5%) were critical access hospitals, 60 (64.5%) were located in micropolitan rural counties; they had a median (IQR) average daily census of 22 (10-53) patients, and 48 (52.2%) had experienced a recent decline in births, with a median (IQR) of 274 (120-446) births in 2019. Respondents reported that the minimum number of annual births needed to safely provide obstetric care was 200 (IQR, 100-350). From a financial perspective, the minimum number of annual births needed was also 200 (IQR, 120-360). When making decisions about maintaining obstetric care, 51 (64.6%) responding hospitals listed their highest priority as meeting local community needs, 13 (16.5%) listed financial considerations, and 10 (12.7%) listed staffing. Overall, 23 (25%) responding hospitals were not sure they would continue providing obstetrics, or they expected to stop offering this service.
Conclusions and relevance: In this survey of US rural hospitals that offer obstetric services, many administrators indicated prioritizing local community needs for obstetric care over concerns about financial viability and staffing.
Copyright 2022 Kozhimannil KB et al. JAMA Health Forum.
Conflict of interest statement
Conflict of Interest Disclosures: Dr Kozhimannil, Ms Interrante, and Dr Admon reported support from the Health Resources and Services Administration PHS Cooperative Agreement No. 5U1CRH03717. Dr Kozhimannil and Dr Basile Ibrahim reported support from the National Institutes of Health National Center for Advancing Translational Sciences, grant UL1TR002494. Dr Admon also reported a grant from AHRQ K08HS027640 during the conduct of the study; as well as grants from National Institutes of Health (NIH) R01MH120124, grants from NIH R01MD014958, grants from the Commonwealth Fund, personal fees from American College of Obstetricians and Gynecologists Consultant, personal fees from Centers for Disease Control and Prevention Consultant, personal fees from Medicaid and CHIP Payment and Access Commission Consultant, and personal fees from NIH.
Figures
References
-
- Ely DM, Driscoll AK. Infant Mortality in the United States, 2018: Data From the Period Linked Birth/Infant Death File. National Center for Health Statistics; 2020:18. - PubMed
