

Racial and Ethnic Disparities in Hospitalization Outcomes Among Medicare Beneficiaries During the COVID-19 Pandemic
- PMID: 35977303
- PMCID: PMC8796953
- DOI: 10.1001/jamahealthforum.2021.4223
Racial and Ethnic Disparities in Hospitalization Outcomes Among Medicare Beneficiaries During the COVID-19 Pandemic
Abstract
Importance: The COVID-19 pandemic has disproportionately affected racial and ethnic minority populations. However, racial and ethnic disparities in hospitalization outcomes during the pandemic-for both COVID-19 and non-COVID-19 hospitalizations-are poorly understood, especially among older populations.
Objective: To assess racial and ethnic differences in hospitalization outcomes during the COVID-19 pandemic among Medicare beneficiaries.
Design setting and participants: In the 100% traditional Medicare inpatient data, there were 31 771 054 unique beneficiaries in cross-section just before the pandemic (February 2020), among whom 26 225 623 were non-Hispanic White, 2 797 462 were Black, 692 994 were Hispanic, and 2 054 975 belonged to other racial and ethnic minority groups. There were 14 021 285 hospitalizations from January 2019 through February 2021, of which 11 353 581 were among non-Hispanic White beneficiaries, 1 656 856 among Black beneficiaries, 321 090 among Hispanic beneficiaries, and 689 758 among beneficiaries of other racial and ethnic minority groups. Sensitivity analyses tested expanded definitions of mortality and alternative model specifications.
Exposures: Race and ethnicity in Medicare claims from the Social Security Administration.
Main outcomes and measures: In-hospital mortality and mortality inclusive of discharges to hospice, deaths during 30-day readmissions, and 30-day all-cause mortality. Secondary outcomes included discharges to hospice and discharges to postacute care.
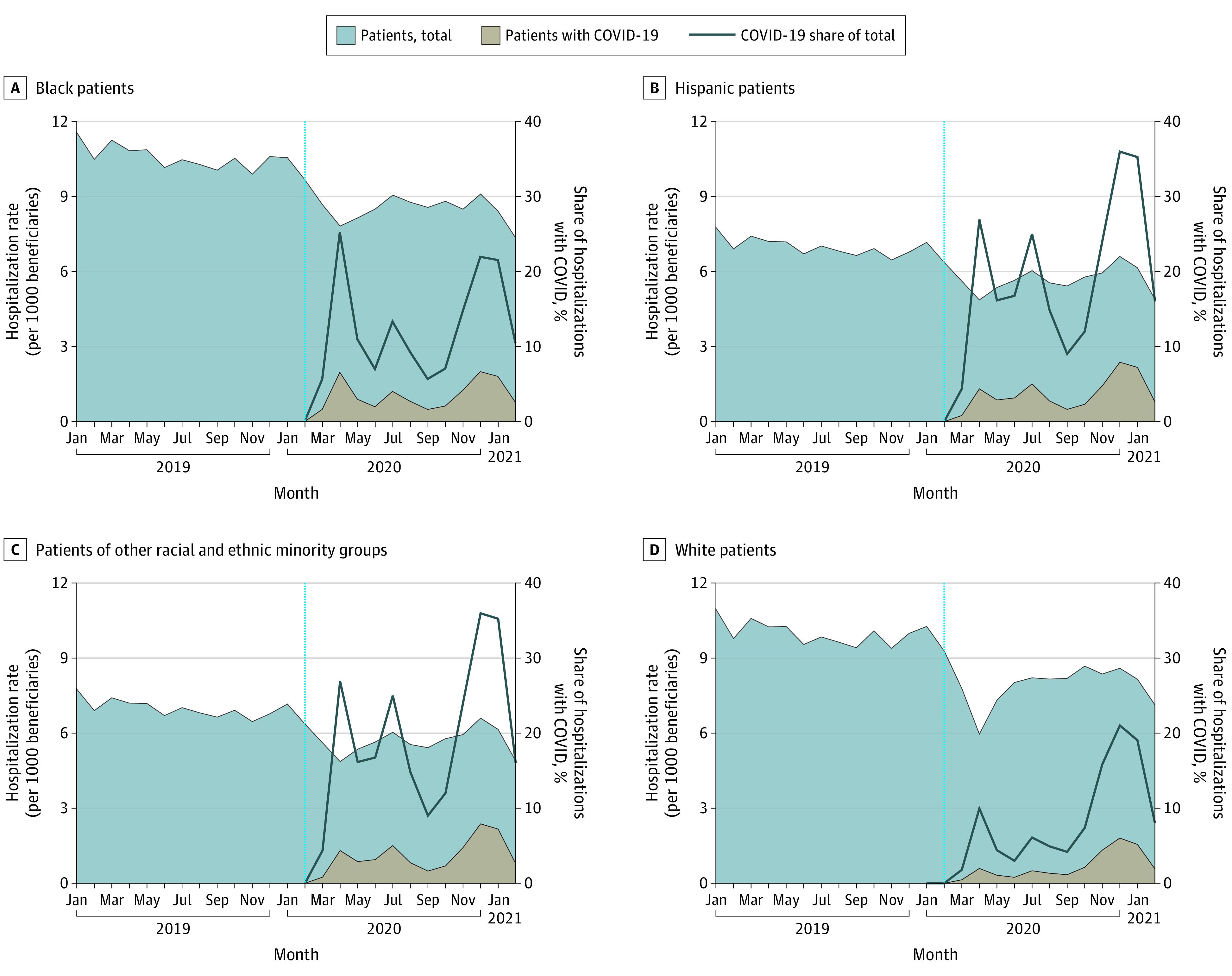
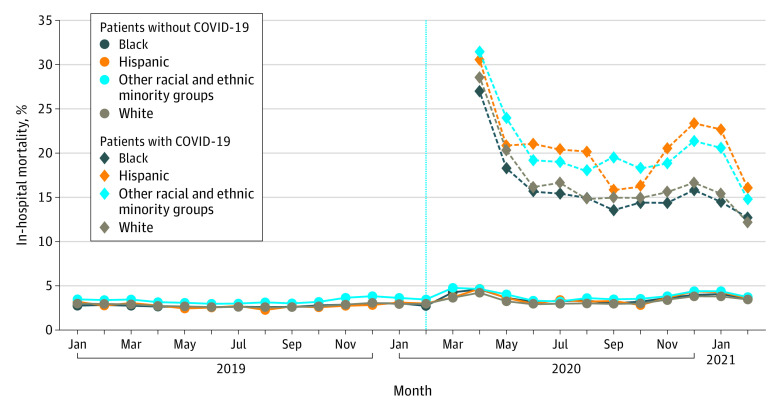
Results: The decline in non-COVID-19 and emergence of COVID-19 hospitalizations were qualitatively similar among beneficiaries of different racial and ethnic minority groups through February 2021. In-hospital COVID-19 mortality was not significantly different among Black patients relative to White patients, but was 3.5 percentage points higher among Hispanic patients (95% CI, 2.9-4.1; P < .001) and other racial and ethnic minority patients relative to White counterparts (95% CI, 3.0-4.1; P < .001). For non-COVID-19 hospitalizations, in-hospital mortality among Black patients increased by 0.5 percentage points more than it increased among White patients (95% CI, 0.3-0.6; P < .001), a 17.5% differential increase relative to the prepandemic baseline. This gap was robust to expanded definitions of mortality. Hispanic patients had similar differential increases in expanded definitions of mortality and model specification. Disparities in discharges to hospice and postacute care were evident. In aggregate across COVID-19 and non-COVID-19 hospitalizations, mortality differentially increased among racial and ethnic minority populations during the pandemic.
Conclusions and relevance: In this cohort study, racial and ethnic disparities in mortality were evident among COVID-19 hospitalizations and widened among non-COVID-19 hospitalizations, motivating greater attention to health equity.
Copyright 2021 Song Z et al. JAMA Health Forum.
Conflict of interest statement
Conflict of Interest Disclosures: Ms Zhang and Mr Haas are employees at Avant-garde Health, which is a health care analytics firm based in Boston, Massachusetts. Dr Lowry Barnes, is the President of the American Association of Hip and Knee Surgeons and holds the Carl L. Nelson, MD, Distinguished Chair in Orthopaedic Surgery in the College of Medicine at the University of Arkansas. His disclosures outside of this work are detailed in the American Association of Hip and Knee Surgeons. No other conflicts were reported.
Figures
Similar articles
-
Racial and Ethnic Differences in Hospice Use and Hospitalizations at End-of-Life Among Medicare Beneficiaries With Dementia.JAMA Netw Open. 2022 Jun 1;5(6):e2216260. doi: 10.1001/jamanetworkopen.2022.16260. JAMA Netw Open. 2022. PMID: 35679046 Free PMC article.
-
Racial and Ethnic Disparities in Buprenorphine and Extended-Release Naltrexone Filled Prescriptions During the COVID-19 Pandemic.JAMA Netw Open. 2022 Jun 1;5(6):e2214765. doi: 10.1001/jamanetworkopen.2022.14765. JAMA Netw Open. 2022. PMID: 35648400 Free PMC article.
-
Racial and Ethnic Disparities in Postpartum Care in the Greater Boston Area During the COVID-19 Pandemic.JAMA Netw Open. 2022 Jun 1;5(6):e2216355. doi: 10.1001/jamanetworkopen.2022.16355. JAMA Netw Open. 2022. PMID: 35737390 Free PMC article.
-
Racial and Ethnic Disparities in COVID-19-Related Infections, Hospitalizations, and Deaths : A Systematic Review.Ann Intern Med. 2021 Mar;174(3):362-373. doi: 10.7326/M20-6306. Epub 2020 Dec 1. Ann Intern Med. 2021. PMID: 33253040 Free PMC article.
-
Racial and ethnic disparities in cardiometabolic disease and COVID-19 outcomes in White, Black/African American, and Latinx populations: Social determinants of health.Prog Cardiovasc Dis. 2022 Mar-Apr;71:4-10. doi: 10.1016/j.pcad.2022.04.004. Epub 2022 Apr 28. Prog Cardiovasc Dis. 2022. PMID: 35490870 Free PMC article. Review.
Cited by
-
Racial and ethnic disparities post-hospitalization for COVID-19: barriers to access to care for survivors of COVID-19 acute respiratory distress syndrome.Sci Rep. 2024 May 21;14(1):11556. doi: 10.1038/s41598-024-61097-0. Sci Rep. 2024. PMID: 38773184 Free PMC article.
-
Evidence on COVID-19 Mortality and Disparities Using a Novel Measure, COVID excess mortality percentage: Evidence from Indiana, Wisconsin, and Illinois.PLoS One. 2024 Jan 31;19(1):e0295936. doi: 10.1371/journal.pone.0295936. eCollection 2024. PLoS One. 2024. PMID: 38295114 Free PMC article.
-
The Relative Importance of Hospital Discharge and Patient Composition in Changing Post-Acute Care Utilization and Outcomes Among Medicare Beneficiaries.Health Serv Insights. 2023 Apr 14;16:11786329231166522. doi: 10.1177/11786329231166522. eCollection 2023. Health Serv Insights. 2023. PMID: 37077324 Free PMC article.
-
Integrated health systems and medical care quality during the COVID-19 pandemic.Health Serv Res. 2025 Jun;60(3):e14433. doi: 10.1111/1475-6773.14433. Epub 2025 Feb 20. Health Serv Res. 2025. PMID: 39976304
-
Race and resource allocation: an online survey of US and UK adults' attitudes toward COVID-19 ventilator and vaccine distribution.BMJ Open. 2022 Nov 21;12(11):e062561. doi: 10.1136/bmjopen-2022-062561. BMJ Open. 2022. PMID: 36410823 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
