

Assessing Catastrophic Health Expenditures Among Uninsured People Who Seek Care in US Hospital-Based Emergency Departments
- PMID: 35977304
- PMCID: PMC8796980
- DOI: 10.1001/jamahealthforum.2021.4359
Assessing Catastrophic Health Expenditures Among Uninsured People Who Seek Care in US Hospital-Based Emergency Departments
Abstract
Importance: Uninsured people uniquely rely on the emergency department (ED) for care as they are less likely to have access to lower-cost alternatives. Prior work has demonstrated that most uninsured patients are at risk of catastrophic health expenditure (CHE) after being hospitalized for life-saving care. The risk of CHE for a single treat-and-release ED visit that does not result in a hospitalization among uninsured patient encounters is currently unknown.
Objective: To estimate the overall national risk of CHE among uninsured patients after a single treat-and-release ED visit from 2006 through 2017, and to characterize this risk across key traits.
Design setting and population: This cross-sectional study is based on a nationally representative sample of hospital-based ED visits between 2006 and 2017 in the United States (US) from the Nationwide Emergency Department Sample (NEDS). It examined outpatient ED visits among uninsured patients.
Main outcomes and measures: Risk of CHE for ED care defined as an ED charge that exceeds 40% of one's estimated annual post-subsistence income.
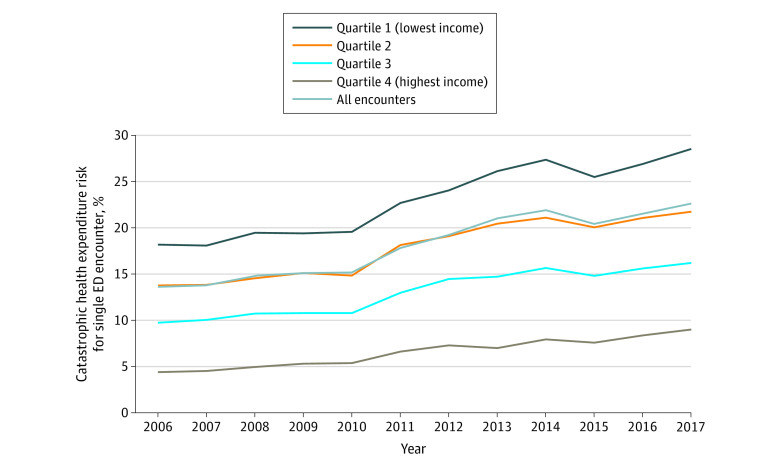
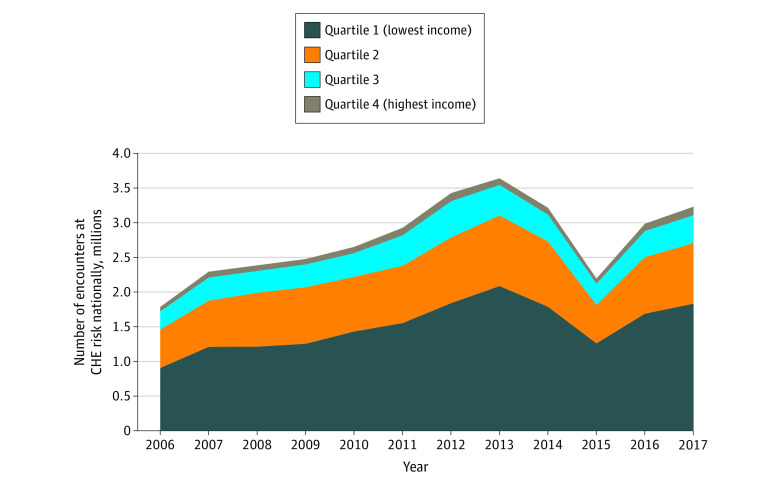
Results: From 2006 to 2017, there were 41.7 million NEDS encounters that met inclusion criteria for this analysis, equating to a nationally weighted estimate of 184.6 million uninsured treat-and-release ED encounters over this period. The median ED charge for a single treat-and-release encounter grew from $842 in 2006 to $2033 by 2017. Approximately 1 in 5 uninsured patients (18% [95% CI, 18.0%-18.0%]) were at risk of CHE for a single treat-and-release ED visit over the study period. This estimated CHE risk increased from 13.6% (95% CI, 13.6%-13.6%) in 2006 to 22.6% (95% CI, 22.6%-22.7%) in 2017. Those living in the lowest income quartile faced a disproportionate share of this risk, with nearly 1 in 3 (28.5% [95% CI, 28.5%-28.6%]) facing CHE risk in 2017. In 2017, an estimated 3.2 million patient encounters nationally were at risk of CHE after a single treat-and-release ED visit.
Conclusions and relevance: This cross-sectional analysis from 2006 to 2017 of 184.6 million uninsured treat-and-release visits found that 1 in 5 uninsured patient encounters are at risk for CHE. This risk has grown over time. Future policies designed to improve access for unscheduled care must consider the unique role of the ED as the de facto safety net and ensure that uninsured patients are not at undue risk of financial harm for seeking care.
Copyright 2021 Scott KW et al. JAMA Health Forum.
Conflict of interest statement
Conflict of Interest Disclosures: Dr K. Scott reported grants from Emergency Medicine Foundation—Society for Academic Emergency Medicine Foundation (EMF-SAEMF) during the conduct of the study. Dr J. Scott reported grants from the Agency for Healthcare Research and Quality and personal fees from BCBS of Michigan during the conduct of the study and salary support from Blue Cross Blue Shield of Michigan through the collaborative quality initiative known as Michigan Social Health Interventions to Eliminate Disparities (MSHIELD) outside the submitted work. Dr Dieleman reported grants from Peterson Center on Healthcare and grants from Gates Ventures during the conduct of the study. No other disclosures were reported.
Figures
Similar articles
-
Outcomes in patients visiting hospital emergency departments in the United States because of periodontal conditions.J Periodontol. 2011 Jun;82(6):809-19. doi: 10.1902/jop.2010.100228. Epub 2010 Dec 7. J Periodontol. 2011. PMID: 21138352
-
US Emergency Department Visits and Hospital Discharges Among Uninsured Patients Before and After Implementation of the Affordable Care Act.JAMA Netw Open. 2019 Apr 5;2(4):e192662. doi: 10.1001/jamanetworkopen.2019.2662. JAMA Netw Open. 2019. PMID: 31002327 Free PMC article.
-
Cured into Destitution: Catastrophic Health Expenditure Risk Among Uninsured Trauma Patients in the United States.Ann Surg. 2018 Jun;267(6):1093-1099. doi: 10.1097/SLA.0000000000002254. Ann Surg. 2018. PMID: 28394867
-
Trends in Emergency Department Use by Rural and Urban Populations in the United States.JAMA Netw Open. 2019 Apr 5;2(4):e191919. doi: 10.1001/jamanetworkopen.2019.1919. JAMA Netw Open. 2019. PMID: 30977849 Free PMC article.
-
Emergency department factors associated with survival after sudden cardiac arrest.Resuscitation. 2013 Mar;84(3):292-7. doi: 10.1016/j.resuscitation.2012.10.013. Epub 2012 Oct 24. Resuscitation. 2013. PMID: 23103887 Review.
Cited by
-
Total and Out-of-Pocket Costs Surrounding Emergency Department Care Among Older Adults Enrolled in Traditional Medicare and Medicare Advantage.Ann Emerg Med. 2024 Sep;84(3):285-294. doi: 10.1016/j.annemergmed.2024.04.023. Epub 2024 Jun 12. Ann Emerg Med. 2024. PMID: 38864783
-
Impact of the Affordable Care Act on Providing Equitable Healthcare Access for IBD in the Kentucky Appalachian Region.Dis Colon Rectum. 2023 Sep 1;66(9):1273-1281. doi: 10.1097/DCR.0000000000002942. Epub 2023 Jun 30. Dis Colon Rectum. 2023. PMID: 37399124 Free PMC article.
-
Prevalence of Chronic Disease and Cost Effectiveness of a Free Clinic.J Community Health. 2025 Apr;50(2):259-269. doi: 10.1007/s10900-024-01417-7. Epub 2024 Oct 19. J Community Health. 2025. PMID: 39425887 Free PMC article.
-
Abdominal Ultrasonography Used for Abdominal Pain in the Rural Outpatient Setting of South Texas: Impact on Patient Outcomes.Cureus. 2024 Jul 13;16(7):e64462. doi: 10.7759/cureus.64462. eCollection 2024 Jul. Cureus. 2024. PMID: 39135831 Free PMC article.
-
Medicaid Enrollment After Hospital Presumptive Eligibility in the Emergency Department.JAMA Health Forum. 2025 Apr 4;6(4):e250768. doi: 10.1001/jamahealthforum.2025.0768. JAMA Health Forum. 2025. PMID: 40279116 Free PMC article.
References
-
- Gonzalez Morganti K, Bauhoff S, Blanchard JC, et al. The Evolving Role of Emergency Departments in the United States. RAND Corporation; 2013. Accessed January 5, 2021. https://www.rand.org/pubs/research_reports/RR280.html - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
