

Measuring the Scope of Prior Authorization Policies: Applying Private Insurer Rules to Medicare Part B
- PMID: 35977311
- PMCID: PMC8796979
- DOI: 10.1001/jamahealthforum.2021.0859
Measuring the Scope of Prior Authorization Policies: Applying Private Insurer Rules to Medicare Part B
Abstract
Importance: Health insurers use prior authorization to evaluate the medical necessity of planned medical services. Data challenges have precluded measuring the frequency with which medical services can require prior authorization, the spending on these services, the types of services and clinician specialties affected, and differences in the scope of prior authorization policies between government-administered and privately administered insurance.
Objectives: To measure the extent of prior authorization requirements for medical services and to describe the services and clinician specialties affected by them using novel data on private insurer coverage policies.
Design setting and participants: Fee-for-service Medicare claims from 2017 were analyzed for beneficiaries in Medicare Part B, which lacks prior authorization. We measured the use of services that would have been subject to prior authorization according to the coverage rules of a large Medicare Advantage insurer and calculated the associated spending. We report the rates of these services for 14 clinical categories and 27 clinician specialties.
Main outcomes and measures: Annual count per beneficiary and associated spending for 1151 services requiring prior authorization by the Medicare Advantage insurer; likelihood of providing 1 or more such service per year, by clinician specialty.
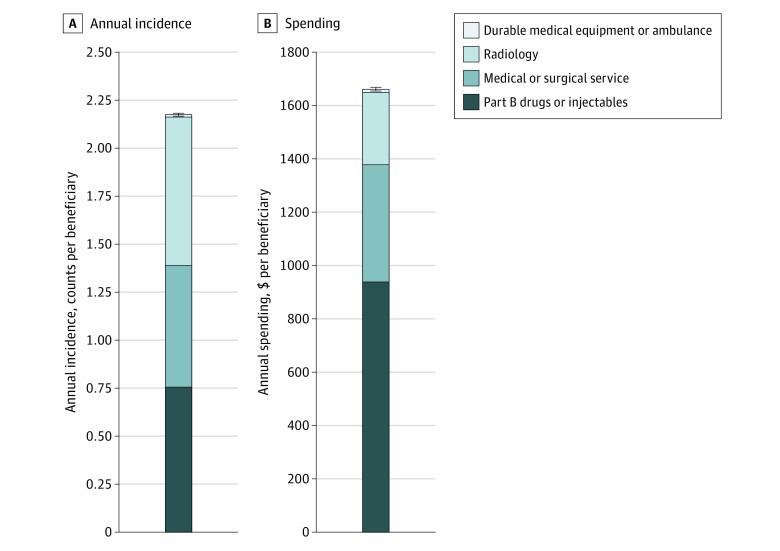
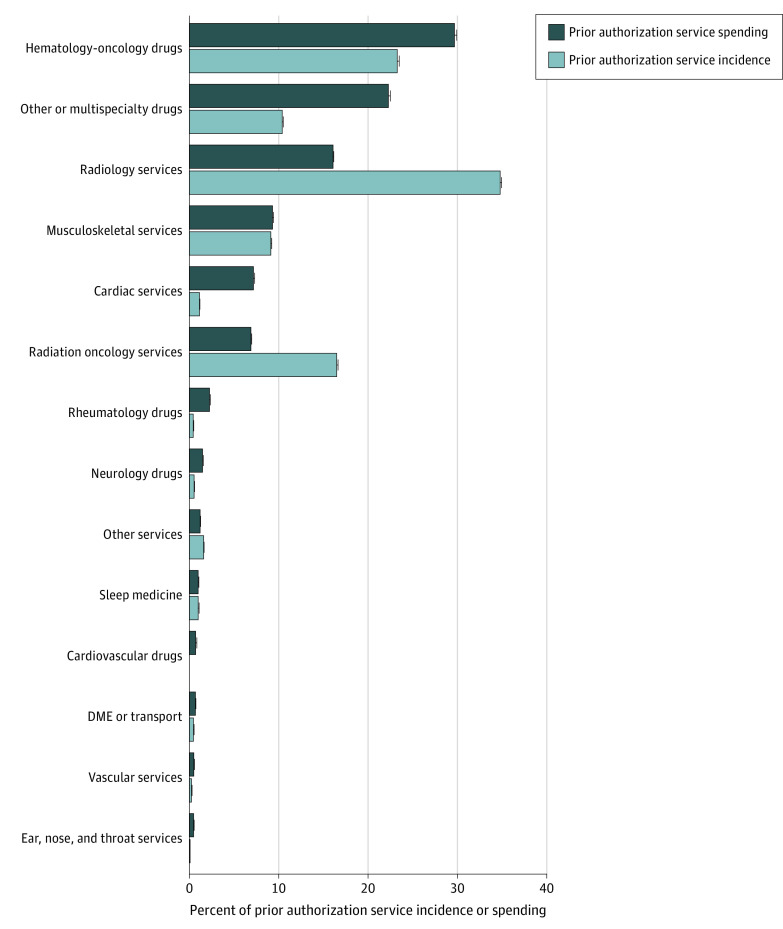
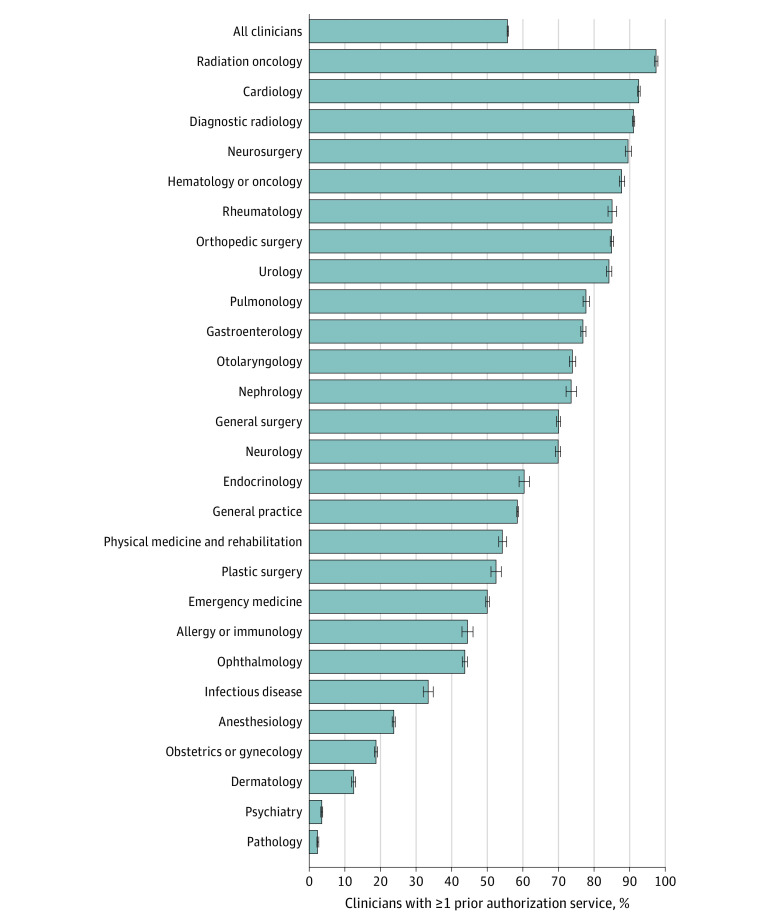
Results: Of 6 497 534 beneficiaries (mean [SD] age, 72.1 [12.1] years), 41% received at least 1 service per year that would have been subject to prior authorization under Medicare Advantage prior authorization requirements. The mean (SD) number of services per beneficiary per year was 2.2 (8.9) (95% CI, 2.17-2.18), corresponding to a mean (SD) of $1661 ($8900) in spending per beneficiary per year (95% CI, $1654-$1668), or 25% of total annual Part B spending. Part B drugs constituted 58% of the associated spending, mostly accounted for by hematology or oncology drugs. Radiology was the largest source of nondrug spending (16%), followed by musculoskeletal services (9%). Physician specialties varied widely in rates of services that required prior authorization, with highest rates among radiation oncologists (97%), cardiologists (93%), and radiologists (91%) and lowest rates among pathologists (2%) and psychiatrists (4%).
Conclusions and relevance: In this cross-sectional study, a large portion of fee-for-service Medicare Part B spending would have been subject to prior authorization under private insurance coverage policies. Prior authorization requirements for Part B drugs have been an important source of difference in coverage policy between government-administered and privately administered Medicare.
Copyright 2021 Schwartz AL et al. JAMA Health Forum.
Conflict of interest statement
Conflict of Interest Disclosures: Dr Schwartz reported receiving personal fees from CVS Health and grants from the Phyllis & Jerome Lyle Rappaport Foundation during the conduct of the study and personal fees from MedPAC, The Lown Institute, and Tufts University School of Medicine outside the submitted work. Dr Brennan reported receiving personal fees from CVS Health during the conduct of the study and outside the submitted work and is employed at CVS Health and has stock and stock options. Dr Newhouse reported receiving personal fees from Aetna and was a director of Aetna through May 2018 and owned Aetna stock through November 2018. No other disclosures were reported.
Figures
Similar articles
-
Comparison of prior authorization across insurers: cross sectional evidence from Medicare Advantage.BMJ. 2024 Mar 7;384:e077797. doi: 10.1136/bmj-2023-077797. BMJ. 2024. PMID: 38453187 Free PMC article.
-
Coverage Denials: Government And Private Insurer Policies For Medical Necessity In Medicare.Health Aff (Millwood). 2022 Jan;41(1):120-128. doi: 10.1377/hlthaff.2021.01054. Health Aff (Millwood). 2022. PMID: 34982629 Free PMC article.
-
Medicare Advantage Prior Authorization Requirements for Otolaryngologic Procedures in 2021.Otolaryngol Head Neck Surg. 2024 Nov;171(5):1601-1604. doi: 10.1002/ohn.931. Epub 2024 Aug 5. Otolaryngol Head Neck Surg. 2024. PMID: 39101347
-
Government and private insurance medical programs as well as MDVIP, an update.J Long Term Eff Med Implants. 2004;14(3):243-50. doi: 10.1615/jlongtermeffmedimplants.v14.i3.80. J Long Term Eff Med Implants. 2004. PMID: 15301667 Review.
-
Medicare in interventional pain management: A critical analysis.Pain Physician. 2006 Jul;9(3):171-97. Pain Physician. 2006. PMID: 16886027 Review.
Cited by
-
Impact of payer rejections and out-of-pocket costs on patient access to bempedoic acid therapy.Am J Prev Cardiol. 2025 Feb 8;21:100940. doi: 10.1016/j.ajpc.2025.100940. eCollection 2025 Mar. Am J Prev Cardiol. 2025. PMID: 40027093 Free PMC article.
-
Differences In Use Of Services And Quality Of Care In Medicare Advantage And Traditional Medicare, 2010 And 2017.Health Aff (Millwood). 2023 Apr;42(4):459-469. doi: 10.1377/hlthaff.2022.00891. Health Aff (Millwood). 2023. PMID: 37011314 Free PMC article.
-
Utilization Management Trends in Medicare Part D Oncology Drugs, 2010-2020.JAMA. 2023 Jul 18;330(3):278-280. doi: 10.1001/jama.2023.10753. JAMA. 2023. PMID: 37462712 Free PMC article.
-
Virtual Radiation Oncology Peer Review is Associated With Decreased Engagement and Limited Case Discussion: Analysis of a Prospective Database Before and During the COVID-19 Pandemic.Int J Radiat Oncol Biol Phys. 2022 Jul 15;113(4):727-731. doi: 10.1016/j.ijrobp.2022.04.026. Epub 2022 Apr 27. Int J Radiat Oncol Biol Phys. 2022. PMID: 35489631 Free PMC article. No abstract available.
-
Comparison of prior authorization across insurers: cross sectional evidence from Medicare Advantage.BMJ. 2024 Mar 7;384:e077797. doi: 10.1136/bmj-2023-077797. BMJ. 2024. PMID: 38453187 Free PMC article.
References
-
- Medicare Payment Advisory Commission . Health Care Spending and the Medicare Program: A Data Book; 2019.
-
- American Hospital Association, America’s Health Insurance Plans, American Medical Association, American Pharmacists Association, BlueCross BlueShield Association, Medical Group Management Associa. Consensus Statement on Improving the Prior Authorization. Published online 2018. Accessed April 21, 2021. https://www.ama-assn.org/sites/ama-assn.org/files/corp/media-browser/pub...
-
- Cutler DM. Reducing Administrative Costs in U.S. Health Care. The Hamilton Project. Accessed October 26, 2020. https://www.hamiltonproject.org/papers/reducing_administrative_costs_in_...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
