

Preventing unrecognised oesophageal intubation: a consensus guideline from the Project for Universal Management of Airways and international airway societies
- PMID: 35977431
- PMCID: PMC9804892
- DOI: 10.1111/anae.15817
Preventing unrecognised oesophageal intubation: a consensus guideline from the Project for Universal Management of Airways and international airway societies
Abstract
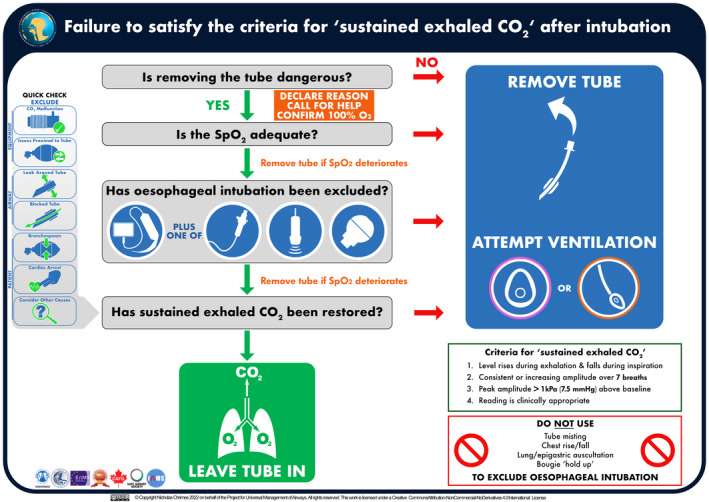
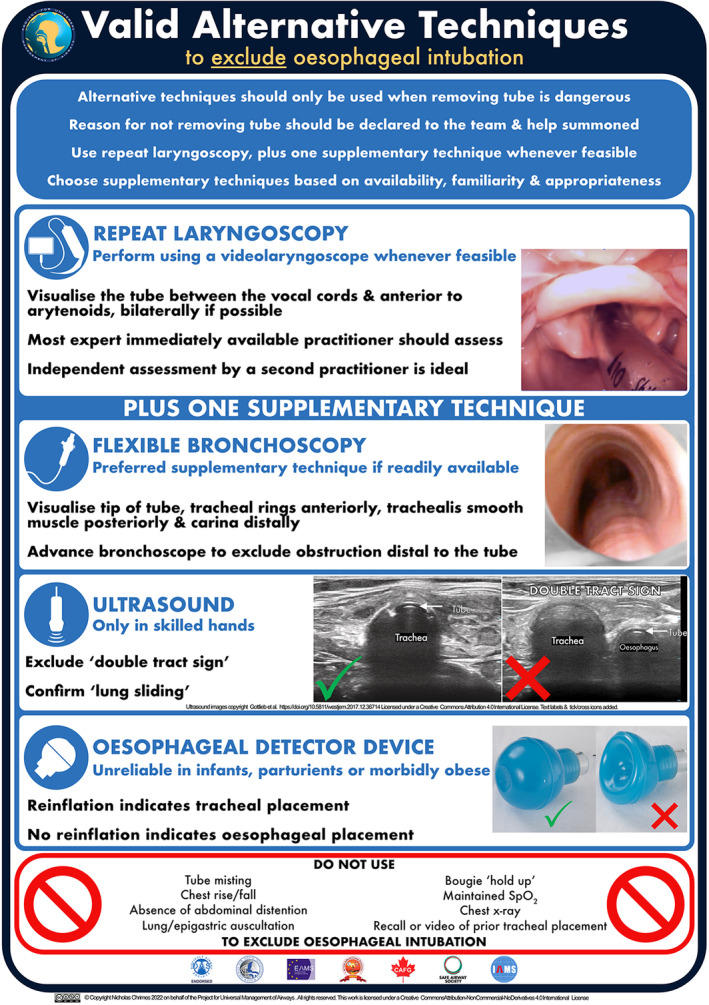
Across multiple disciplines undertaking airway management globally, preventable episodes of unrecognised oesophageal intubation result in profound hypoxaemia, brain injury and death. These events occur in the hands of both inexperienced and experienced practitioners. Current evidence shows that unrecognised oesophageal intubation occurs sufficiently frequently to be a major concern and to merit a co-ordinated approach to address it. Harm from unrecognised oesophageal intubation is avoidable through reducing the rate of oesophageal intubation, combined with prompt detection and immediate action when it occurs. The detection of 'sustained exhaled carbon dioxide' using waveform capnography is the mainstay for excluding oesophageal placement of an intended tracheal tube. Tube removal should be the default response when sustained exhaled carbon dioxide cannot be detected. If default tube removal is considered dangerous, urgent exclusion of oesophageal intubation using valid alternative techniques is indicated, in parallel with evaluation of other causes of inability to detect carbon dioxide. The tube should be removed if timely restoration of sustained exhaled carbon dioxide cannot be achieved. In addition to technical interventions, strategies are required to address cognitive biases and the deterioration of individual and team performance in stressful situations, to which all practitioners are vulnerable. These guidelines provide recommendations for preventing unrecognised oesophageal intubation that are relevant to all airway practitioners independent of geography, clinical location, discipline or patient type.
Keywords: airway management; capnography; human factors; oesophageal intubation; tracheal intubation.
© 2022 The Authors. Anaesthesia published by John Wiley & Sons Ltd on behalf of Association of Anaesthetists.
Figures

Comment in
-
PUMA guideline for preventing unrecognised oesophageal intubation.Anaesthesia. 2023 Jan;78(1):127. doi: 10.1111/anae.15871. Epub 2022 Sep 21. Anaesthesia. 2023. PMID: 36130831 No abstract available.
-
Prevention of unrecognised oesophageal intubation and associated patient harm.Anaesthesia. 2023 Jan;78(1):129-130. doi: 10.1111/anae.15880. Epub 2022 Oct 6. Anaesthesia. 2023. PMID: 36203335 No abstract available.
-
How rapid is rapid enough? Time as an overlooked component of anaesthetic interventions.Anaesthesia. 2023 Jan;78(1):131-132. doi: 10.1111/anae.15882. Epub 2022 Oct 7. Anaesthesia. 2023. PMID: 36205234 No abstract available.
-
Preventing unrecognised oesophageal intubation: addressing hierarchies and the importance of critical language.Anaesthesia. 2023 Jan;78(1):130-131. doi: 10.1111/anae.15891. Epub 2022 Oct 18. Anaesthesia. 2023. PMID: 36256690 No abstract available.
-
Recognising oesophageal intubation.Anaesthesia. 2022 Dec;77(12):1321-1325. doi: 10.1111/anae.15894. Epub 2022 Nov 4. Anaesthesia. 2022. PMID: 36330952 No abstract available.
-
PUMA guidelines for preventing unrecognised oesophageal intubation: don't forget the oxygen.Anaesthesia. 2023 Mar;78(3):399-400. doi: 10.1111/anae.15915. Epub 2022 Nov 12. Anaesthesia. 2023. PMID: 36371528 No abstract available.
-
Dubito ergo sum. From philosophy towards prevention of unrecognised oesophageal intubation.Eur J Anaesthesiol. 2023 May 1;40(5):310-312. doi: 10.1097/EJA.0000000000001822. Eur J Anaesthesiol. 2023. PMID: 37017357 No abstract available.
References
-
- Apfelbaum JL, Hagberg CA, Connis RT, et al. 2022 American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway. Anesthesiology 2022; 136: 31–81. - PubMed
-
- Japanese Society of Anesthesiologists . JSA airway management guideline 2014: to improve the safety of induction of anesthesia. Journal of Anesthesia 2014; 28: 482–93. - PubMed
-
- British Association of Perinatal Medicine . Managing the difficult airway in the neonate. https://www.bapm.org/resources/199‐managing‐the‐difficult‐airway‐in‐the‐... (accessed 28/12/2021).
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
