

Nivolumab plus rucaparib for metastatic castration-resistant prostate cancer: results from the phase 2 CheckMate 9KD trial
- PMID: 35977756
- PMCID: PMC9389086
- DOI: 10.1136/jitc-2022-004761
Nivolumab plus rucaparib for metastatic castration-resistant prostate cancer: results from the phase 2 CheckMate 9KD trial
Abstract
Background: CheckMate 9KD (NCT03338790) is a non-randomized, multicohort, phase 2 trial of nivolumab plus other anticancer treatments for metastatic castration-resistant prostate cancer (mCRPC). We report results from cohorts A1 and A2 of CheckMate 9KD, specifically evaluating nivolumab plus rucaparib.
Methods: CheckMate 9KD enrolled adult patients with histologically confirmed mCRPC, ongoing androgen deprivation therapy, and an Eastern Cooperative Oncology Group performance status of 0-1. Cohort A1 included patients with postchemotherapy mCRPC (1-2 prior taxane-based regimens) and ≤2 prior novel hormonal therapies (eg, abiraterone, enzalutamide, apalutamide); cohort A2 included patients with chemotherapy-naïve mCRPC and prior novel hormonal therapy. Patients received nivolumab 480 mg every 4 weeks plus rucaparib 600 mg two times per day (nivolumab dosing ≤2 years). Coprimary endpoints were objective response rate (ORR) per Prostate Cancer Clinical Trials Working Group 3 and prostate-specific antigen response rate (PSA50-RR; ≥50% PSA reduction) in all-treated patients and patients with homologous recombination deficiency (HRD)-positive tumors, determined before enrollment. Secondary endpoints included radiographic progression-free survival (rPFS), overall survival (OS), and safety.
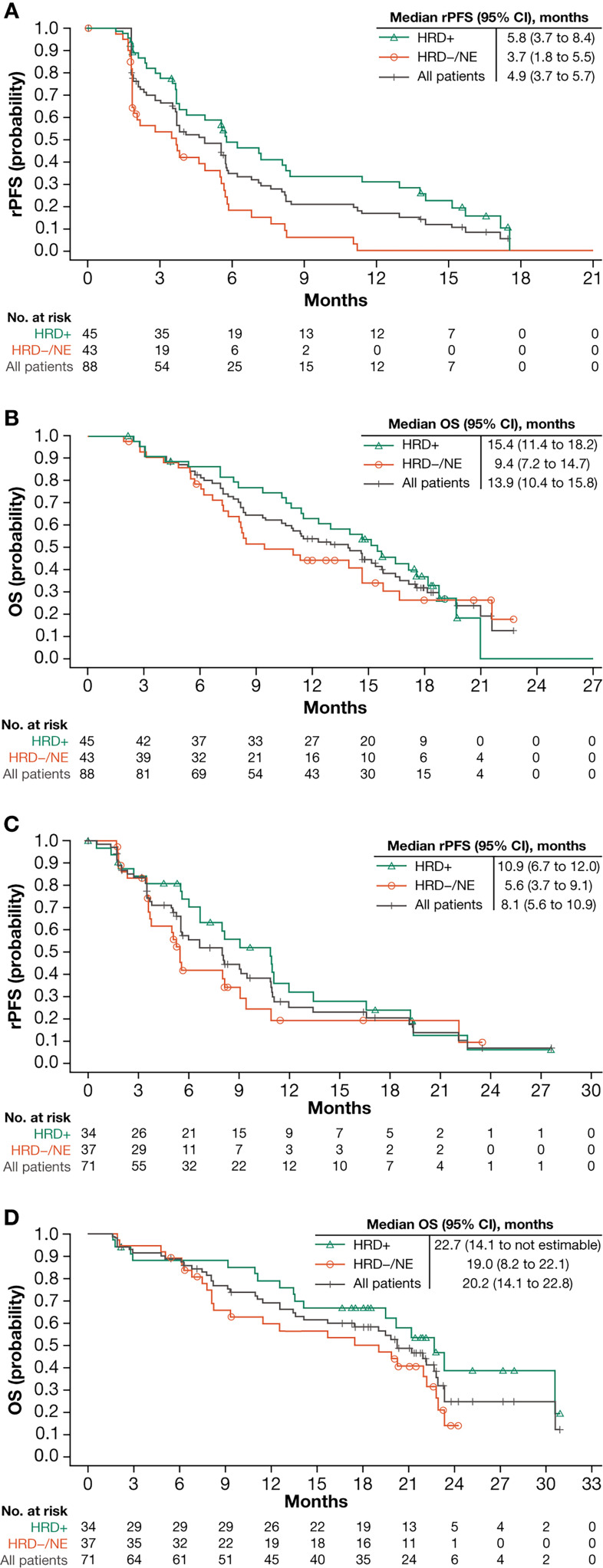
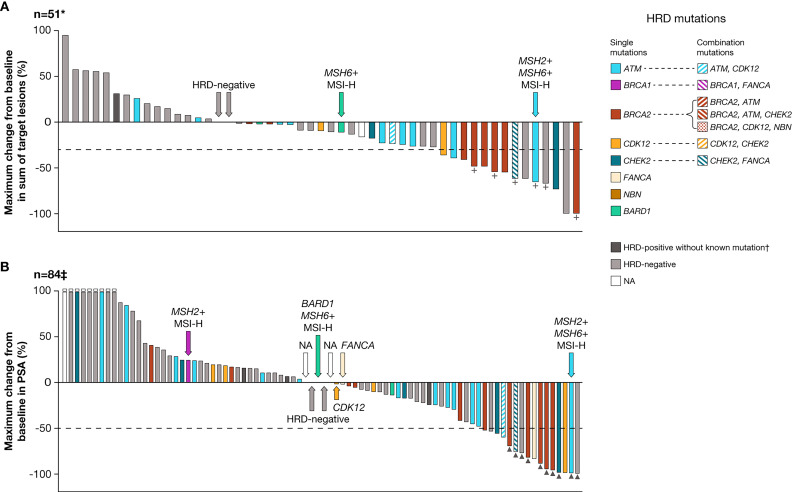
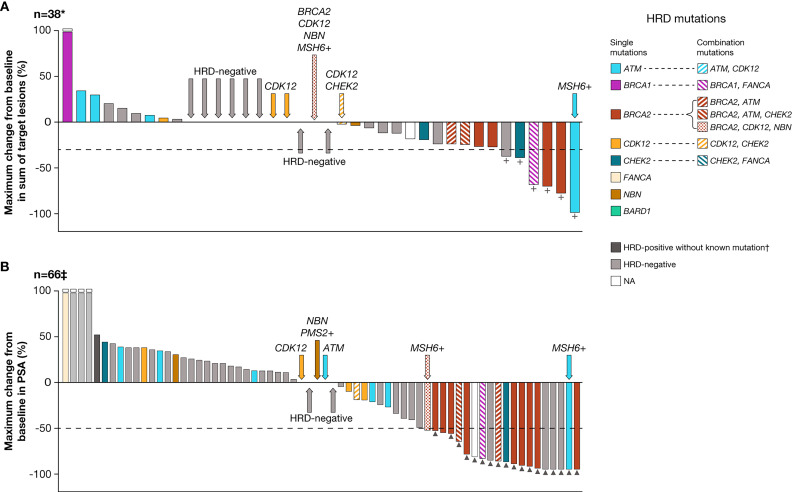
Results: Outcomes (95% CI) among all-treated, HRD-positive, and BRCA1/2-positive populations for cohort A1 were confirmed ORR: 10.3% (3.9-21.2) (n=58), 17.2% (5.8-35.8) (n=29), and 33.3% (7.5-70.1) (n=9); confirmed PSA50-RR: 11.9% (5.9-20.8) (n=84), 18.2% (8.2-32.7) (n=44), and 41.7% (15.2-72.3) (n=12); median rPFS: 4.9 (3.7-5.7) (n=88), 5.8 (3.7-8.4) (n=45), and 5.6 (2.8-15.7) (n=12) months; and median OS: 13.9 (10.4-15.8) (n=88), 15.4 (11.4-18.2) (n=45), and 15.2 (3.0-not estimable) (n=12) months. For cohort A2 they were confirmed ORR: 15.4% (5.9-30.5) (n=39), 25.0% (8.7-49.1) (n=20), and 33.3% (7.5-70.1) (n=9); confirmed PSA50-RR: 27.3% (17.0-39.6) (n=66), 41.9 (24.5-60.9) (n=31), and 84.6% (54.6-98.1) (n=13); median rPFS: 8.1 (5.6-10.9) (n=71), 10.9 (6.7-12.0) (n=34), and 10.9 (5.6-12.0) (n=15) months; and median OS: 20.2 (14.1-22.8) (n=71), 22.7 (14.1-not estimable) (n=34), and 20.2 (11.1-not estimable) (n=15) months. In cohorts A1 and A2, respectively, the most common any-grade and grade 3-4 treatment-related adverse events (TRAEs) were nausea (40.9% and 40.8%) and anemia (20.5% and 14.1%). Discontinuation rates due to TRAEs were 27.3% and 23.9%, respectively.
Conclusions: Nivolumab plus rucaparib is active in patients with HRD-positive postchemotherapy or chemotherapy-naïve mCRPC, particularly those harboring BRCA1/2 mutations. Safety was as expected, with no new signals identified. Whether the addition of nivolumab incrementally improves outcomes versus rucaparib alone cannot be determined from this trial.
Trial registration number: NCT03338790.
Keywords: Clinical Trials, Phase II as Topic; Immunotherapy.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: KF reports advisory board fees (all institutional) from Amgen, Astellas, AstraZeneca, Bayer, Clovis, Janssen, MSD, Novartis/AAA, Sanofi, CureVac, and Orion. MR reports research grants (all institutional) from Bristol Myers Squibb (BMS) and Janssen; speakers bureau fees from Astellas, BMS, Janssen, Merck, MSD, and Roche; and advisory board fees from Astellas, Janssen, Merck, MSD, and Roche. DPP reports consulting fees from Ada Cap, Amgen, Astellas, AstraZeneca, Bayer, Bicycle Therapeutics, Boehringer Ingelheim, BMS, Clovis Oncology, Exelixis, Gilead Sciences, Incyte, Ipsen, Johnson & Johnson/Janssen, Lilly, Mirati, Monopteros, Pfizer, Pharmacyclics, Regeneron, Roche, Seattle Genetics, and UroGen; stock ownership in Bellicum Pharmaceuticals and Tyme; payment for expert testimony from Sanofi and Celgene; research grants from Ada Cap, Agensys, Astellas Pharma, AstraZeneca, Bayer, BioXcel Therapeutics, BMS, Clovis Oncology, Eisai, Endocyte, Genentech, Gilead Sciences, Innocrin, Lilly, MedImmune, Medivation, Merck, Mirati, Novartis, Pfizer, Progenics, Replimune, Roche, Sanofi Aventis, and Seattle Genetics; local principal investigator (PI) nonfinancial interests (all institutional) in Ada Cap, Agensys, Inc., Astellas, AstraZeneca, Bayer, BioXcel Therapeutics, BMS, Clovis Oncology, Eisai, Eli Lilly, Endocyte, Genentech, Innocrin, MedImmune, Medivation, Merck, Mirati, Novartis, and Pfizer; medical writing support from Bioscript; study funding from Astellas; and editing support from Complete HealthVizion. JCG reports consulting fees from Eisai; honoraria from AstraZeneca, BMS, Ipsen, and MSD Australia, advisory board fees from BMS and Janssen (J&J); and stock ownership in ICON Cancer Care. JP-G reports research funding (all institutional) from BMS, Amgen, Roche, and Seattle Genetics; travel expenses from Roche, BMS, and MSD; and advisory board fees from BMS, Roche, Ipsen, Seattle Genetics, and MSD. LL reports local PI nonfinancial (all institutional) from Astellas, AstraZeneca, Bayer, BMS, Hoffman-La Roche, Janssen, MedImmune, Merck, Myovant, Pfizer, Sanofi and Telix. SZ reports research grants (institutional) from Eisai; speakers bureau fees from Eisai (personal) and Merck (institutional); honoraria for educational events from Eisai, Ipsen, Merck, MSD, and Pfizer; travel expenses from Celgene (institutional); advisory board fees from Amgen, Bayer, and Sanofi (personal), and Astellas, BMS, EUSA, Merck, MSD, Pfizer, and Roche, (all institutional); receipt of drugs (institutional) from KURA; local PI nonfinancial interests from Astellas, Bayer, Calithera Biosciences, Clovis Oncology, Exelixis, Sanofi/Aventis, and SEAGEN; and coordinating PI nonfinancial interests from AVEO Pharmaceuticals, BMS, Pfizer, and Roche. MB reports consulting fees from AstraZeneca, BMS, MSD Oncology, Novartis, and Roche/Genentech; and speakers bureau fees from AstraZeneca, BMS, MSD Oncology, and Roche/Genentech. HM reports travel expenses from Pfizer and Roche, advisory board fees from Astellas, Bayer, BMS, Janssen, MSD, Pfizer, Sanofi, AstraZeneca, and Roche; and PI nonfinancial interests from BMS, Janssen, MSD, Pfizer, Roche, and Sanofi. GG reports research funding (institutional) from BMS; speakers bureau fees (all institutional) from Amgen, Astellas Pharma, BMS, Ipsen, Janssen Oncology, MSD Oncology, and Sanofi/Aventis; travel expenses from Astellas Pharma, AstraZeneca, BMS, Ipsen, Janssen Oncology, and Sanofi; and advisory board fees (all institutional) from AstraZeneca, Bayer, BMS, Ipsen, Janssen, MSD Oncology, Pfizer, and Sanofi/Aventis. DAB reports research grants (all institutional) from Astellas, Bayer, and Janssen; speakers bureau fees from AstraZeneca, Bayer, BMS, Janssen, Merck, MSD, and Roche; and advisory board fees from Astellas, Bayer, Janssen. SLM reports speakers bureau fees from BMS; and local PI nonfinancial interests (all institutional) from BMS, Merck, and Roche/Genentech. JCVL reports employment from Hospital Civil de Guadalajara 'Fray Antonio Alcalde'; and local PI nonfinancial interests (all personal and institutional) from AstraZeneca, BMS, Europharma, Janssen, MSD, and Novartis. EMK reports speakers bureau fees from Astellas Pharma, Ipsen, and Janssen; writing engagement fees from Research Review; and local PI nonfinancial interests (all institutional) from Astellas Pharma, AstraZeneca, BMS, Merck KGaA, and Pfizer. DC reports consulting fees from Astellas Pharma, AstraZeneca, Bayer, Boehringer Ingelheim, BMS, Ipsen, Janssen Oncology, Lilly, MSD Oncology, Novartis, Pfizer, Pierre Fabre, Roche/Genentech, and Sanofi; travel expenses from AstraZeneca Spain, BMS, Pfizer, and Roche; and research funding (institutional) from Janssen. AF reports honoraria from Astellas Pharma, AstraZeneca, Bayer, BMS, Ipsen, Janssen-Cilag, MSD Oncology, Pfizer, Roche/Genentech, and Sanofi/Aventis; and travel expenses from Astellas Pharma, AstraZeneca, Bayer, BMS, Ipsen, Janssen-Cilag, MSD Oncology, Pfizer, Roche/Genentech, and Sanofi/Aventis. FS reports research grants (all institutional) from Astellas, AstraZeneca, BMS, Janssen, Merck, Myovant, Novartis, Pfizer, and Sanofi; consulting fees from Astellas, AstraZeneca, Janssen, Merck, Myovant, Novartis, Pfizer, and Sanofi; honoraria from Astellas, AstraZeneca, Janssen, Merck, Novartis, Pfizer, and Sanofi; advisory board fees from Astellas, Bayer, BMS, Janssen, Myovant, Novartis, and Pfizer; and local PI nonfinancial interests (all institutional) from Amgen, Astellas, Bayer, BMS, Janssen, Novartis, Pfizer, and Sanofi. M-OG reports trial funding and medical writing funding from BMS, research funding (institutional) from BMS and Intuitive Surgical; consulting fees from Astellas Pharma, AstraZeneca, Bayer Vital, BMS, Eisai, EUSA Pharma, Ipsen, Merck Serono, MSD, Pfizer, Roche Pharma AG, and Takeda; honoraria from Astellas Pharma, AstraZeneca, BMS, EUSA Pharma, Ipsen, Merck Serono, MSD, and Pfizer; and travel expenses from BMS and Merck Serono. DRS has no competing interest to report. AJA reports research funding and writing grant (institutional) from BMS; consulting fees from Astellas, AstraZeneca, Bayer, BMS, Dendreon, Exelixis, Forma, Janssen, Merck, Myovant, Novartis/AAA, and Pfizer; advisory board fees from AstraZeneca, Bayer, Dendreon, Merck, Myovant, Novartis/AAA, and Pfizer; local PI nonfinancial interests (institutional) from Amgen, Bayer, BeiGene, Merck, Forma, and AstraZeneca; coordinating PI nonfinancial interests (institutional) from Astellas, BMS, Janssen, and Pfizer; and steering committee member nonfinancial interests (institutional) from Dendreon. PB reports employment from and stock ownership in BMS. NPA reports employment from and stock ownership in BMS. KU-K reports employment from and stock ownership in BMS at the time of the study. KU-K is now employed by BioNTech US. XW reports employment from and stock ownership in BMS at the time of the study, and stock ownership in AstraZeneca. XW is no longer employed by BMS. JL reports employment from and stock ownership in BMS. AL reports employment from and stock ownership in Clovis Oncology. RKP reports research funding (institutional) from Janssen and Pharmacyclics; speakers bureau fees from AstraZeneca, Genentech/Roche, and Sanofi; advisory board fees from Bayer, BMS, Dendreon, EMD Serono, Genomic Health, Janssen, Jounce, and Pfizer; PI nonfinancial interests from BMS, ESSA, Janssen, Merck, and Pfizer/EMD Serono; steering committee member nonfinancial interests from BMS; and licensed technology to Tempus Labs.
Figures
Comment in
-
Urologic Oncology: Prostate Cancer.J Urol. 2023 Apr;209(4):807-809. doi: 10.1097/JU.0000000000003180. Epub 2023 Jan 25. J Urol. 2023. PMID: 36695094 No abstract available.
References
-
- National Comprehensive Cancer Network (NCCN) . Clinical practice guidelines in oncology: prostate cancer. Version 1, 2022.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous