

Clinical and Structural Findings in Patients With Lesion-Induced Dystonia: Descriptive and Quantitative Analysis of Published Cases
- PMID: 35977840
- PMCID: PMC9651464
- DOI: 10.1212/WNL.0000000000201042
Clinical and Structural Findings in Patients With Lesion-Induced Dystonia: Descriptive and Quantitative Analysis of Published Cases
Abstract
Background and objectives: Brain lesions are a well-recognized etiology of dystonia. These cases are especially valuable because they offer causal insight into the neuroanatomical substrates of dystonia. To date, knowledge of lesion-induced dystonia comes mainly from isolated case reports or small case series, restricting broader description and analysis.
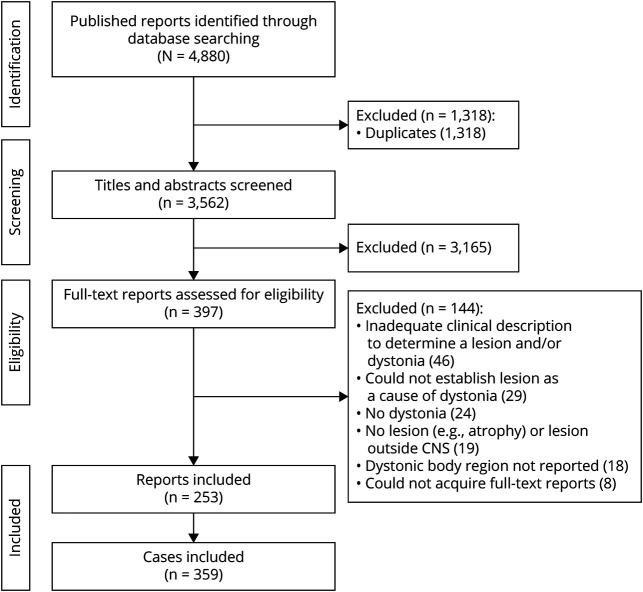
Methods: Cases of lesion-induced dystonia were first identified from a systematic review of published literature. Latent class analysis then investigated whether patients could be classified into subgroups based on lesion location and body regions affected by dystonia. Regression analyses subsequently investigated whether subgroup membership predicted clinical characteristics of dystonia.
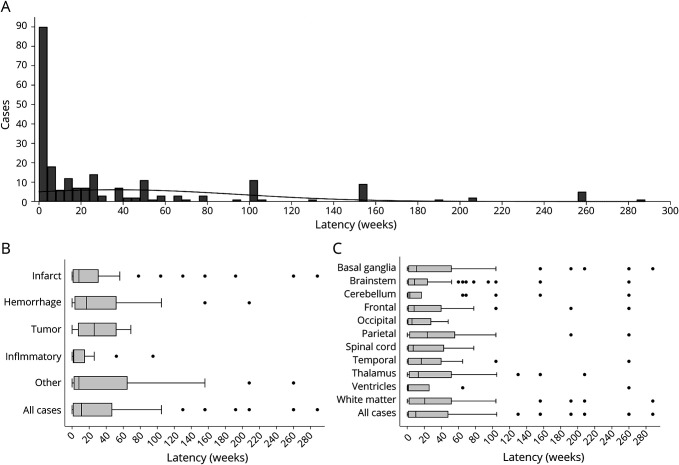
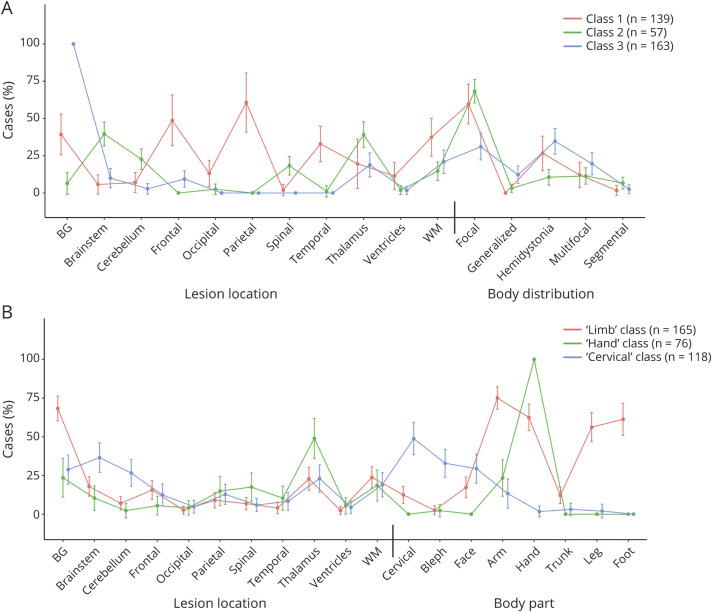
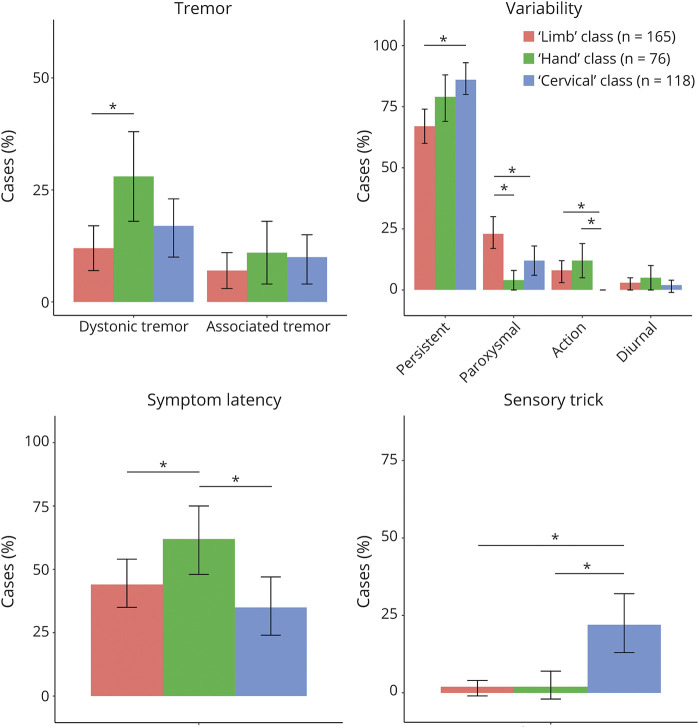
Results: Three hundred fifty-nine published cases were included. Lesions causing dystonia occurred in heterogeneous locations, most commonly in the basal ganglia (46.2%), followed by the thalamus (28.1%), brainstem (22.6%), and white matter (21.2%). The most common form of lesion-induced dystonia was focal dystonia (53.2%), with the hand (49.9%) and arm (44.3%) most commonly affected. Of all cases, 86.6% reported co-occurring neurologic manifestations and 26.1% reported other movement disorders. Latent class analysis identified 3 distinct subgroups of patients: those with predominantly limb dystonias, which were associated with basal ganglia lesions; those with hand dystonia, associated with thalamic lesions; and those with predominantly cervical dystonia, associated with brainstem and cerebellar lesions. Regression demonstrated significant differences between these subgroups on a range of dystonia symptoms, including dystonic tremor, symptom latency, other movement disorders, and dystonia variability.
Discussion: Although dystonia can be induced by lesions to numerous brain regions, there are distinct relationships between lesion locations and dystonic body parts. This suggests that the affected brain networks are different between types of dystonia.
© 2022 American Academy of Neurology.
Figures
Comment in
-
Lesion-Induced Dystonia: Lessons Learned From Brain Network Studies.Neurology. 2022 Nov 1;99(18):777-778. doi: 10.1212/WNL.0000000000201266. Epub 2022 Aug 17. Neurology. 2022. PMID: 35977834 No abstract available.
References
-
- LeDoux MS, Brady KA. Secondary cervical dystonia associated with structural lesions of the central nervous system. Mov Disord. 2003;18(1):60-69. - PubMed
-
- Galardi G, Perani D, Grassi F, et al. Basal ganglia and thalamo-cortical hypermetabolism in patients with spasmodic torticollis. Acta Neurol Scand. 1996;94(3):172-176. - PubMed
-
- Naumann M, Pirker W, Reiners K, Lange KW, Becker G, Brücke T. Imaging the pre-and postsynaptic side of striatal dopaminergic synapses in idiopathic cervical dystonia: a SPECT STUDY Using [123I] epidepride and [123I] β-CIT. Mov Disord. 1998;13(2):319-323. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical