Effect of prone positioning on gas exchange according to lung morphology in patients with acute respiratory distress syndrome
- PMID: 35977897
- PMCID: PMC9475165
- DOI: 10.4266/acc.2022.00367
Effect of prone positioning on gas exchange according to lung morphology in patients with acute respiratory distress syndrome
Abstract
Background: There are limited data on the clinical effects of prone positioning according to lung morphology. We aimed to determine whether the gas exchange response to prone positioning differs according to lung morphology.
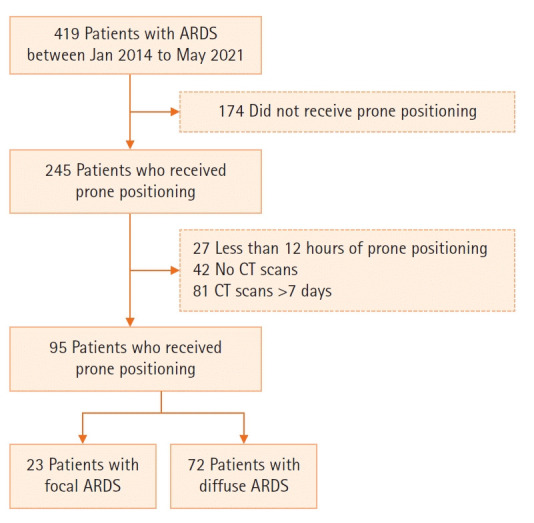
Methods: This retrospective study included adult patients with moderate-to-severe acute respiratory distress syndrome (ARDS). The lung morphology of ARDS was assessed by chest computed tomography scan and classified as "diffuse" or "focal." The primary outcome was change in partial pressure of arterial oxygen to fraction of inspired oxygen (PaO2/FiO2) ratio after the first prone positioning session: first, using the entire cohort, and second, using subgroups of patients with diffuse ARDS matched 2 to 1 with patients with focal ARDS at baseline.
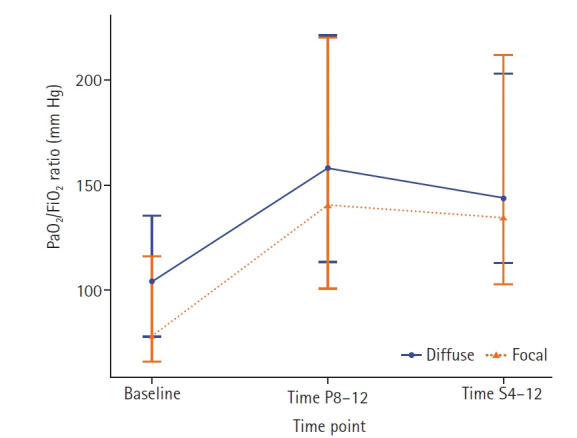
Results: Ninety-five patients were included (focal ARDS group, 23; diffuse ARDS group, 72). Before prone positioning, the focal ARDS group showed worse oxygenation than the diffuse ARDS group (median PaO2/FiO2 ratio, 79.9 mm Hg [interquartile range (IQR)], 67.7-112.6 vs. 104.0 mm Hg [IQR, 77.6-135.7]; P=0.042). During prone positioning, the focal ARDS group showed a greater improvement in the PaO2/FiO2 ratio than the diffuse ARDS group (median, 55.8 mm Hg [IQR, 11.1-109.2] vs. 42.8 mm Hg [IQR, 11.6-83.2]); however, the difference was not significant (P=0.705). Among the PaO2/FiO2-matched cohort, there was no significant difference in change in PaO2/FiO2 ratio after prone positioning between the groups (P=0.904).
Conclusions: In patients with moderate-to-severe ARDS, changes in PaO2/FiO2 ratio after prone positioning did not differ according to lung morphology. Therefore, prone positioning can be considered as soon as indicated, regardless of ARDS lung morphology.
Keywords: acute respiratory distress syndrome; dynamic compliance of lung; lung morphology; oxygenation; prone positioning.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Effect of prone positioning on oxygenation and static respiratory system compliance in COVID-19 ARDS vs. non-COVID ARDS.Respir Res. 2021 Aug 6;22(1):220. doi: 10.1186/s12931-021-01819-4. Respir Res. 2021. PMID: 34362368 Free PMC article. Review.
-
Respiratory Physiology of Prone Positioning With and Without Inhaled Nitric Oxide Across the Coronavirus Disease 2019 Acute Respiratory Distress Syndrome Severity Spectrum.Crit Care Explor. 2021 Jun 15;3(6):e0471. doi: 10.1097/CCE.0000000000000471. eCollection 2021 Jun. Crit Care Explor. 2021. PMID: 34151287 Free PMC article.
-
Combined effects of prone positioning and airway pressure release ventilation on gas exchange in patients with acute lung injury.Acta Anaesthesiol Scand. 2003 May;47(5):516-24. doi: 10.1034/j.1399-6576.2003.00109.x. Acta Anaesthesiol Scand. 2003. PMID: 12699507 Clinical Trial.
-
Prone positioning in mechanically ventilated patients with severe acute respiratory distress syndrome and coronavirus disease 2019.Acta Anaesthesiol Scand. 2021 Mar;65(3):360-363. doi: 10.1111/aas.13741. Epub 2020 Nov 22. Acta Anaesthesiol Scand. 2021. PMID: 33165936 Free PMC article.
-
Acute Respiratory Distress Syndrome: Advances in Diagnosis and Treatment.JAMA. 2018 Feb 20;319(7):698-710. doi: 10.1001/jama.2017.21907. JAMA. 2018. PMID: 29466596 Review.
Cited by
-
Subphenotypes of Acute Respiratory Distress Syndrome: Advancing Towards Precision Medicine.Tuberc Respir Dis (Seoul). 2024 Jan;87(1):1-11. doi: 10.4046/trd.2023.0104. Epub 2023 Sep 7. Tuberc Respir Dis (Seoul). 2024. PMID: 37675452 Free PMC article.
-
Imaging and pulmonary function techniques in ARDS diagnosis and management: current insights and challenges.Crit Care. 2025 Jul 6;29(1):282. doi: 10.1186/s13054-025-05520-6. Crit Care. 2025. PMID: 40619387 Free PMC article. Review.
References
-
- Ashbaugh DG, Bigelow DB, Petty TL, Levine BE. Acute respiratory distress in adults. Lancet. 1967;2:319–23. - PubMed
-
- Acute Respiratory Distress Syndrome Network. Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, et al. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342:1301–8. - PubMed
-
- Papazian L, Forel JM, Gacouin A, Penot-Ragon C, Perrin G, Loundou A, et al. Neuromuscular blockers in early acute respiratory distress syndrome. N Engl J Med. 2010;363:1107–16. - PubMed
-
- Briel M, Meade M, Mercat A, Brower RG, Talmor D, Walter SD, et al. Higher vs lower positive end-expiratory pressure in patients with acute lung injury and acute respiratory distress syndrome: systematic review and meta-analysis. JAMA. 2010;303:865–73. - PubMed
LinkOut - more resources
Full Text Sources