Effect of a nutritional support protocol on enteral nutrition and clinical outcomes of critically ill patients: a retrospective cohort study
- PMID: 35977898
- PMCID: PMC9475161
- DOI: 10.4266/acc.2022.00220
Effect of a nutritional support protocol on enteral nutrition and clinical outcomes of critically ill patients: a retrospective cohort study
Abstract
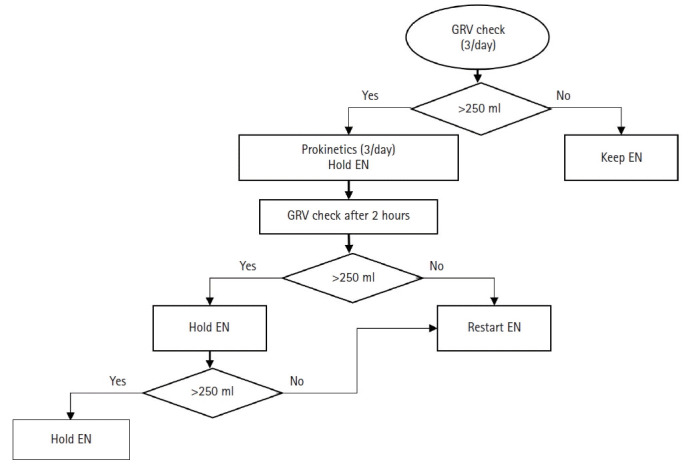
Background: Enteral nutrition (EN) supply within 48 hours after intensive care unit (ICU) admission improves clinical outcomes. The "new ICU evaluation & development of nutritional support protocol (NICE-NST)" was introduced in an ICU of tertiary academic hospital. This study showed that early EN through protocolized nutritional support would supply more nutrition to improve clinical outcomes.
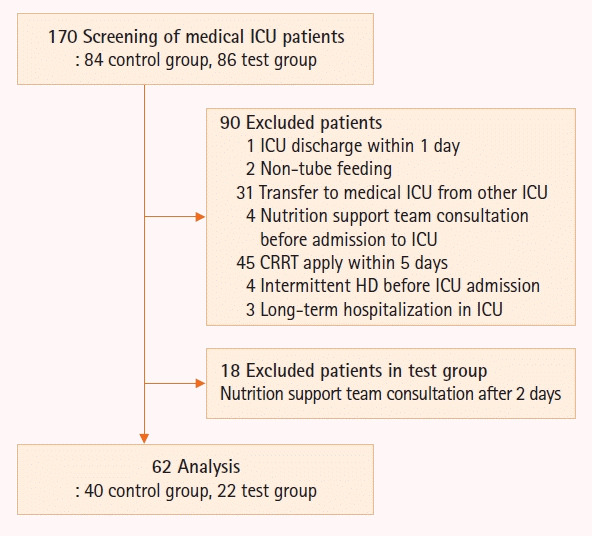
Methods: This study screened 170 patients and 62 patients were finally enrolled; patients who were supplied nutrition without the protocol were classified as the control group (n=40), while those who were supplied according to the protocol were classified as the test group (n=22).
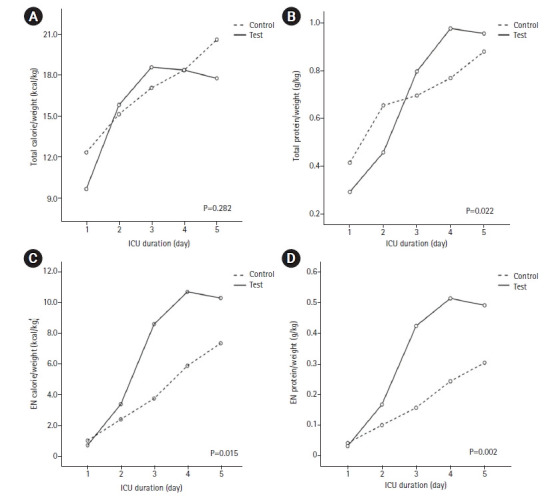
Results: In the test group, EN started significantly earlier (3.7±0.4 days vs. 2.4±0.5 days, P=0.010). EN calorie (4.0±1.0 kcal/kg vs. 6.7±0.9 kcal/kg, P=0.006) and protein (0.17±0.04 g/kg vs. 0.32±0.04 g/kg, P=0.002) supplied were significantly higher in the test group. Although EN was supplied through continuous feeding in the test group, there was no difference in complications such as feeding hold due to excessive gastric residual volume or vomit, and hyper- or hypo-glycemia between the two groups. Hospital mortality was significantly lower in the group that started EN within 1.5 days (42.9% vs. 11.8%, P=0.018). The proportion of patients who started EN within 1.5 days was higher in the test group (40.9% vs. 17.5%, P=0.044).
Conclusions: The NICE-NST may improve EN supply and mortality of critically ill patients without increasing complications.
Keywords: clinical protocols; complications; critical care outcomes; critical illness; enteral nutrition; nutritional support.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Feeding the critically ill obese patient: a systematic review protocol.JBI Database System Rev Implement Rep. 2015 Oct;13(10):95-109. doi: 10.11124/jbisrir-2015-2458. JBI Database System Rev Implement Rep. 2015. PMID: 26571286
-
Route of nutrition and risk of blood stream infections in critically ill patients; a comparative study.Clin Nutr ESPEN. 2016 Apr;12:e14-e19. doi: 10.1016/j.clnesp.2016.01.002. Epub 2016 Mar 2. Clin Nutr ESPEN. 2016. PMID: 28531664
-
Canadian clinical practice guidelines for nutrition support in mechanically ventilated, critically ill adult patients.JPEN J Parenter Enteral Nutr. 2003 Sep-Oct;27(5):355-73. doi: 10.1177/0148607103027005355. JPEN J Parenter Enteral Nutr. 2003. PMID: 12971736
-
The impact of implementation of an enteral feeding protocol on the improvement of enteral nutrition in critically ill adults.Asia Pac J Clin Nutr. 2017 Jan;26(1):27-35. doi: 10.6133/apjcn.122015.01. Asia Pac J Clin Nutr. 2017. PMID: 28049258 Review.
-
Meeting nutritional targets of critically ill patients by combined enteral and parenteral nutrition: review and rationale for the EFFORTcombo trial.Nutr Res Rev. 2020 Dec;33(2):312-320. doi: 10.1017/S0954422420000165. Epub 2020 Jul 16. Nutr Res Rev. 2020. PMID: 32669140 Review.
Cited by
-
Effect of nutrition support team on 28-day mortality in Korean patients with acute respiratory failure.Acute Crit Care. 2025 May;40(2):313-321. doi: 10.4266/acc.003312. Epub 2025 Apr 28. Acute Crit Care. 2025. PMID: 40302562 Free PMC article.
References
-
- Kreymann KG, Berger MM, Deutz NE, Hiesmayr M, Jolliet P, Kazandjiev G, et al. ESPEN guidelines on enteral nutrition: intensive care. Clin Nutr. 2006;25:210–23. - PubMed
-
- Dhaliwal R, Cahill N, Lemieux M, Heyland DK. The Canadian critical care nutrition guidelines in 2013: an update on current recommendations and implementation strategies. Nutr Clin Pract. 2014;29:29–43. - PubMed
-
- Taylor BE, McClave SA, Martindale RG, Warren MM, Johnson DR, Braunschweig C, et al. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.) Crit Care Med. 2016;44:390–438. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials