

Clinical characteristics, causes and predictors of outcomes in patients with in-hospital cardiac arrest: results from the SURVIVE-ARREST study
- PMID: 35978110
- PMCID: PMC9898362
- DOI: 10.1007/s00392-022-02084-1
Clinical characteristics, causes and predictors of outcomes in patients with in-hospital cardiac arrest: results from the SURVIVE-ARREST study
Abstract
Introduction: In-hospital cardiac arrest (IHCA) is acutely life-threatening and remains associated with high mortality and morbidity. Identifying predictors of mortality after IHCA would help to guide acute therapy.
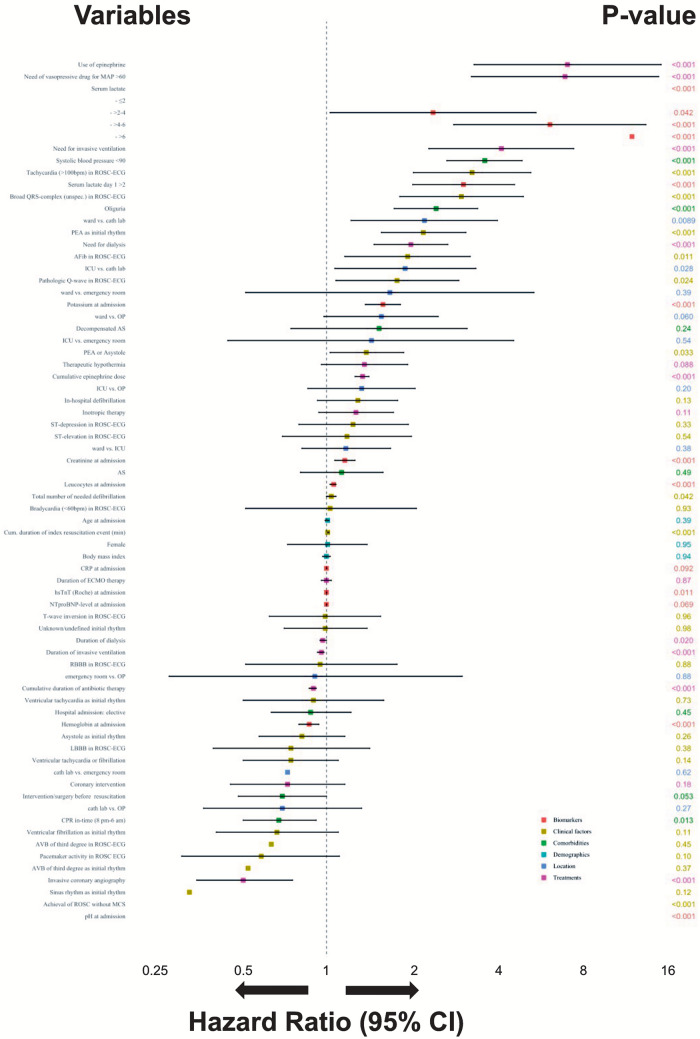
Methods: We determined patient characteristics and independent predictors of 30-day in-hospital mortality, neurological outcome, and discharge/referral pathways in patients experiencing IHCA in a large tertiary care hospital between January 2014 and April 2017. Multivariable Cox regression model was fitted to assess predictors of outcomes.
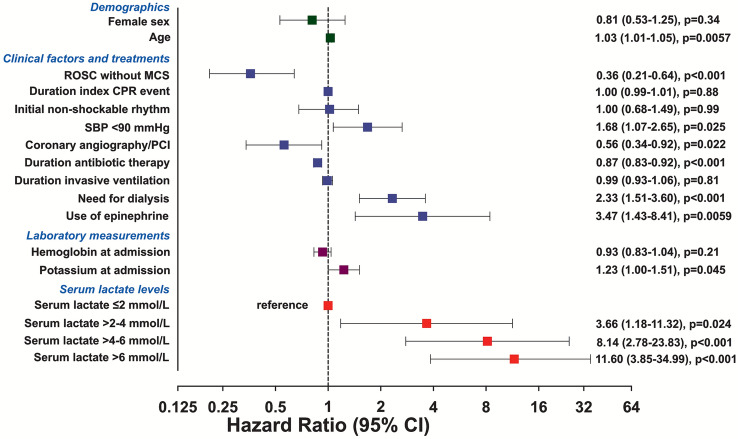
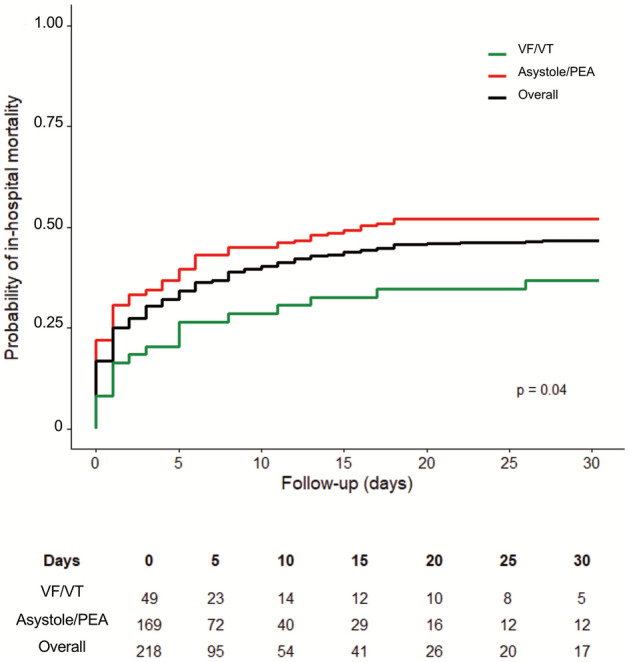
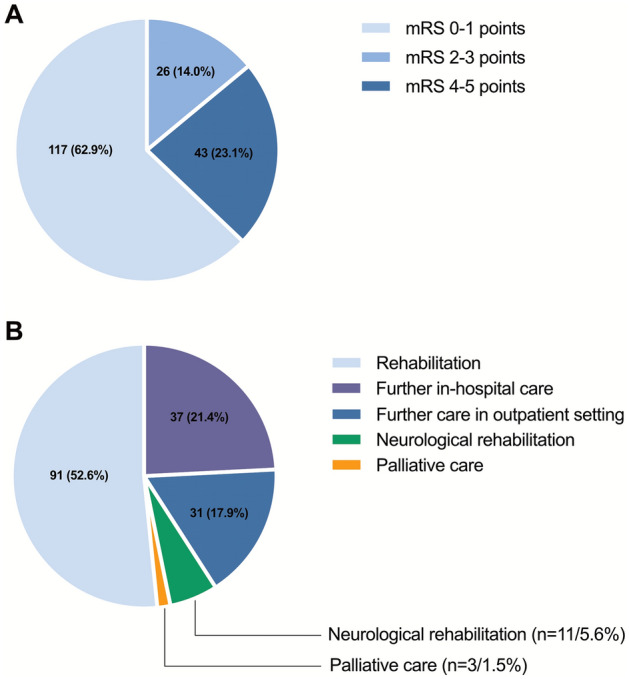
Results: A total of 368 patients with IHCA were analysed (median age 73 years (interquartile range 65-78), 123 (33.4%) women). Most patients (45.9%) had an initial non-shockable rhythm and shockable rhythms were found in 20.9%; 23.6% of patients suffered from a recurrent episode of cardiac arrest. 172/368 patients died within 30 days (46.7%). Of 196/368 patients discharged alive after IHCA, the majority (72.9%, n = 143) had a good functional neurological outcome (modified Rankin Scale ≤ 3 points). In the multivariable analysis, return of spontaneous circulation without mechanical circulatory support (hazard ratio (HR) 0.36, 95% confidence interval (CI) 0.21-0.64), invasive coronary angiography and/or percutaneous intervention (HR 0.56, 95% CI 0.34-0.92), and antibiotic therapy (HR 0.87, 95% CI 0.83-0.92) were associated with a lower risk of 30-day in hospital mortality.
Conclusion: In the present study, IHCA was survived in ~ 50% in a tertiary care hospital, although only a minority of patients presented with shockable rhythms. The majority of IHCA survivors (~ 70%) had a good neurological outcome. Recovery of spontaneous circulation and presence of treatable acute causes of the arrest are associated with better survival. Clinical Characteristics, Causes and Predictors of Outcomes in Patients with In-Hospital Cardiac Arrest: Results from the SURVIVE-ARREST Study.
Abbreviations: CPR, cardiopulmonary resuscitation; IHCA, In-hospital cardiac arrest; MCS, mechanical circulatory support; PCI, percutaneous coronary intervention; ROSC, return of spontaneous circulation; SBP, systolic blood pressure.
Keywords: Hospitalization; In-hospital cardiac arrest; Mortality; Outcomes; Survival.
© 2022. The Author(s).
Conflict of interest statement
Dr. Becher was partially supported by the German Research Foundation (Grant number BE 7424/2-1). Dr. Schrage received funding from the German Research Foundation and the Else Kröner-Fresenius-Stiftung, and speakers fees from Astra Zeneca, outside from the submitted work. Dr. Toprak receives funding for a research project by the German Foundation of Heart Research outside the submitted work. Dr. Kluge received research support from Cytosorbents and Daiichi Sankyo. He also received lecture fees from Astra, Bard, Baxter, Biotest, Cytosorbents, Daiichi Sankyo, Fresenius Medical Care, Gilead, Mitsubishi Tanabe Pharma, MSD, Pfizer, Philips and Zoll. He received consultant fees from Fresenius, Gilead, MSD and Pfizer. Dr. Blankenberg reports grants from Abbott Diagnostics, Siemens, Singulex, grants and personal fees from Bayer, Thermofisher, personal fees from Novartis, outside the submitted work; and payments or honoraria for lectures, presentations, speaker bureaus, manuscript writing or educational events, support for attending meetings and travel from Abbott, AstraZeneca, Bayer, Amgen, Medtronic, Pfizer, Siemens and Thermofisher, all outside the submitted work. Dr. Kirchhof was partially supported by European Union BigData@Heart (grant agreement EU IMI 116074), AFFECT-AF (grant agreement 847770), and MAESTRIA (grant agreement 965286), British Heart Foundation (AA/18/2/34218), German Center for Cardiovascular Research supported by the German Ministry of Education and Research (DZHK), and Leducq Foundation. PK receives research support for basic, translational, and clinical research projects from European Union, British Heart Foundation, Leducq Foundation, Medical Research Council (UK), and German Centre for Cardiovascular Research, from several drug and device companies active in atrial fibrillation and has received honoraria from several such companies in the past, but not in the last three years. PK is listed as inventor on two patents held by University of Birmingham (Atrial Fibrillation Therapy WO 2015140571, Markers for Atrial Fibrillation WO 2016012783). Dr. Clemmensen reports personal fees from Abbott, Acarix, AstraZeneca, Aventis, Bayer, Boehringer Ingelheim, Bristol Myers Squibb, Daiichi Sankyo, Eli Lilly, Evolva, Fibrex, Janssen, Merck, Myogen, Medtronic, Mitsubishi Pharma, The Medicines Company, Nycomed, Organon, Pfizer, Pharmacia, Regado, Sanofi, Searle, and Servier, all outside the submitted work. Dr. Sinning received fees from AstraZeneca and Johnson&Johnson, all outside the submitted work. Dr. Zengin-Sahm received fees from AstraZeneca, all outside the submitted work. Dr. Hannen, Dr. Fluschnik, Dr. Issleib, Dr. Roedl, Dr. Söffker, Mrs. Mahmoodi, Mrs. Weimann have no COI to declare.
Figures
References
-
- Chan PS, Tang Y, American Heart Association's Get With the Guidelines-Resuscitation I Risk-standardizing rates of return of spontaneous circulation for in-hospital cardiac arrest to facilitate hospital comparisons. J Am Heart Assoc. 2020;9(7):e014837. doi: 10.1161/JAHA.119.014837. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
