

Outcomes and prognostic factors in patients with locally advanced cervical cancer treated with concurrent chemoradiotherapy
- PMID: 35978412
- PMCID: PMC9386993
- DOI: 10.1186/s13014-022-02115-1
Outcomes and prognostic factors in patients with locally advanced cervical cancer treated with concurrent chemoradiotherapy
Abstract
Background: To investigate the prognostic factors affecting long-term survival in locally advanced cervical cancer (LACC) patients treated with concurrent chemoradiotherapy (CCRT).
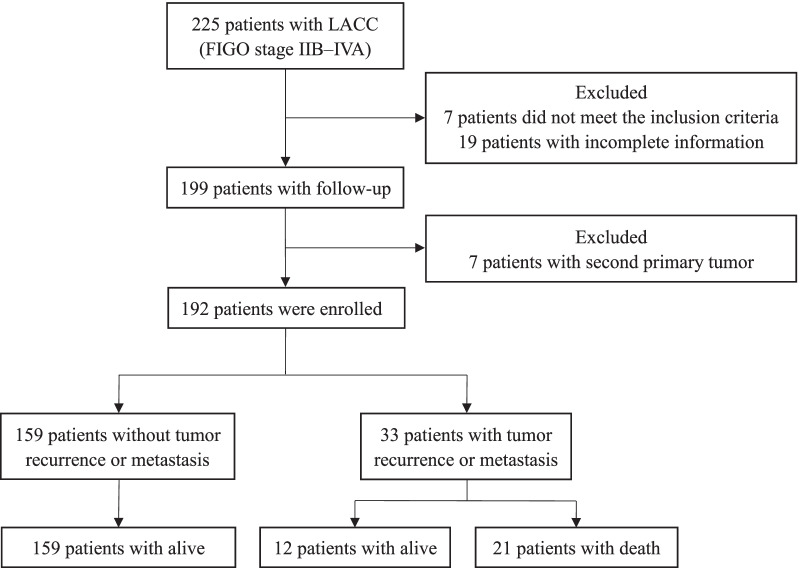
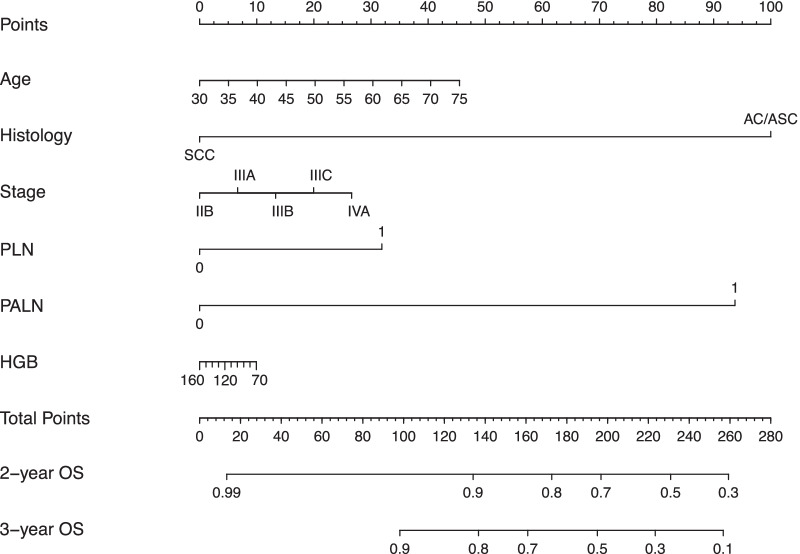
Methods: We retrospectively analyzed 192 naive LACC (stage IIB-IVA) patients who underwent intensity-modulated radiotherapy (IMRT) with concurrent platinum-based chemotherapy in Xiangya Hospital from January 2014 to June 2017. The clinicopathological factors of all patients were collected. To explore the relationship between factors and prognosis, survival rates were estimated by the Kaplan-Meier method. Univariate and multivariate Cox proportional hazards models were used to evaluate the effect of various factors on overall survival (OS) and progression-free survival (PFS). The nomogram and calibration curves were generated on the basis of survival analysis.
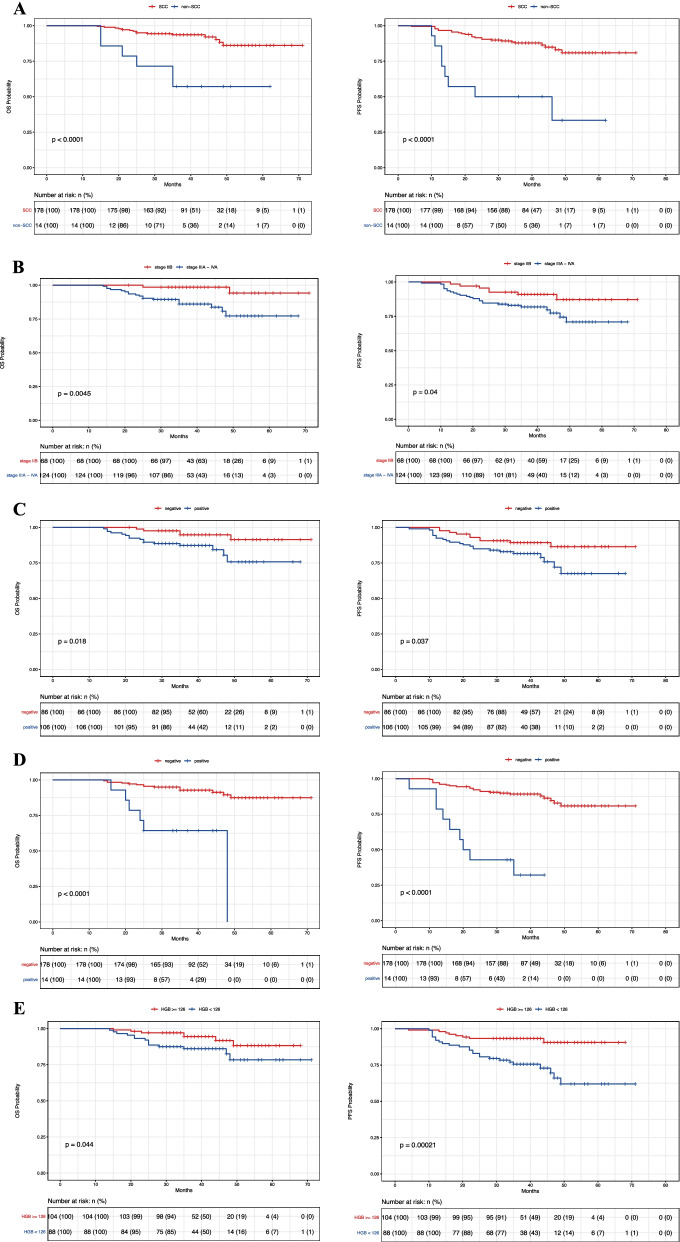
Results: The median follow-up time was 39.5 months. There-year rates of OS and PFS were 89.1% and 82.8%. LACC patients with non-squamous cell carcinoma [NSCC, including adenocarcinoma or adenosquamous carcinoma (AC/ASC)], advanced stage (IIIA-IVA), initially positive lymph node (pelvic or para-aortic lymph node, PLN/PALN), and a lower pretreatment hemoglobin (HGB) level (< 126 g/L) had lower survival rates. In univariate analysis, patients with NSCC, advanced stage, PLN or PALN metastasis had worse OS. Patients with NSCC, advanced stage, PLN or PALN metastasis, and a lower pretreatment HGB level had worse PFS. In multivariate analysis, NSCC and PALN metastasis were independent prognostic parameters of OS. NSCC, PALN metastasis and a lower pretreatment HGB level were independent prognostic parameters of PFS.
Conclusions: NSCC and PALN metastasis were poor prognostic factors of OS and PFS, a lower pretreatment HGB level was an independent prognostic factor of PFS in LACC patients treated with CCRT.
Keywords: Concurrent chemoradiotherapy; Locally advanced cervical cancer; Prognostic factors; Recurrence or metastasis.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
Nomogram for Predicting Survival in Locally Advanced Cervical Cancer with Concurrent Chemoradiotherapy plus or Not Adjuvant Chemotherapy: A Retrospective Analysis Based on 2018 FIGO Staging.Cancer Biother Radiopharm. 2024 Nov;39(9):690-705. doi: 10.1089/cbr.2023.0199. Epub 2024 Jun 3. Cancer Biother Radiopharm. 2024. PMID: 38828494
-
[Outcomes and prognostic factors of distant metastasis in patients with advanced cervical squamous cell carcinoma treated with concurrent chemoradiotherapy].Zhonghua Fu Chan Ke Za Zhi. 2015 Feb;50(2):125-30. Zhonghua Fu Chan Ke Za Zhi. 2015. PMID: 25877610 Chinese.
-
The prognostic factors for locally advanced cervical cancer patients treated by intensity-modulated radiation therapy with concurrent chemotherapy.J Formos Med Assoc. 2015 Mar;114(3):231-7. doi: 10.1016/j.jfma.2012.10.021. Epub 2013 Jan 5. J Formos Med Assoc. 2015. PMID: 25777974
-
Hyperfractionated radiotherapy with concurrent chemotherapy for para-aortic lymph node recurrence in carcinoma of the cervix.Int J Radiat Oncol Biol Phys. 2003 Apr 1;55(5):1247-53. doi: 10.1016/s0360-3016(02)04401-2. Int J Radiat Oncol Biol Phys. 2003. PMID: 12654434 Review.
-
Efficacy and safety of chemoradiotherapy plus immune checkpoint inhibitors for the treatment of locally advanced cervical cancer: a systematic review and meta-analysis.Front Immunol. 2024 Sep 16;15:1459693. doi: 10.3389/fimmu.2024.1459693. eCollection 2024. Front Immunol. 2024. PMID: 39351236 Free PMC article.
Cited by
-
Targeting autophagy promotes the antitumor effect of radiotherapy on cervical cancer cells.Cancer Biol Ther. 2024 Dec 31;25(1):2431136. doi: 10.1080/15384047.2024.2431136. Epub 2024 Dec 5. Cancer Biol Ther. 2024. PMID: 39635971 Free PMC article.
-
Hematologic Toxicity Profiles and the Impact of Hemoglobin Nadir and Transfusion on Oncologic Outcome in Definitive Radiochemotherapy for Cervical Cancer.Cancers (Basel). 2024 Nov 27;16(23):3986. doi: 10.3390/cancers16233986. Cancers (Basel). 2024. PMID: 39682174 Free PMC article.
-
Can we triumph over locally advanced cervical cancer with colossal para-aortic lymph nodes? A case report.World J Clin Cases. 2024 Apr 6;12(10):1851-1856. doi: 10.12998/wjcc.v12.i10.1851. World J Clin Cases. 2024. PMID: 38660077 Free PMC article.
-
Prediction of Recurrent Cervical Cancer in 2-Year Follow-Up After Treatment Based on Quantitative and Qualitative Magnetic Resonance Imaging Parameters: A Preliminary Study.Ann Surg Oncol. 2023 Sep;30(9):5577-5585. doi: 10.1245/s10434-023-13756-1. Epub 2023 Jun 25. Ann Surg Oncol. 2023. PMID: 37355522
-
Immunotherapy in cervical cancer: From the view of scientometric analysis and clinical trials.Front Immunol. 2023 Feb 3;14:1094437. doi: 10.3389/fimmu.2023.1094437. eCollection 2023. Front Immunol. 2023. PMID: 36817443 Free PMC article. Clinical Trial.
