

Arterial spin labeling and diffusion-weighted imaging for identification of retropharyngeal lymph nodes in patients with nasopharyngeal carcinoma
- PMID: 35978445
- PMCID: PMC9387018
- DOI: 10.1186/s40644-022-00480-4
Arterial spin labeling and diffusion-weighted imaging for identification of retropharyngeal lymph nodes in patients with nasopharyngeal carcinoma
Abstract
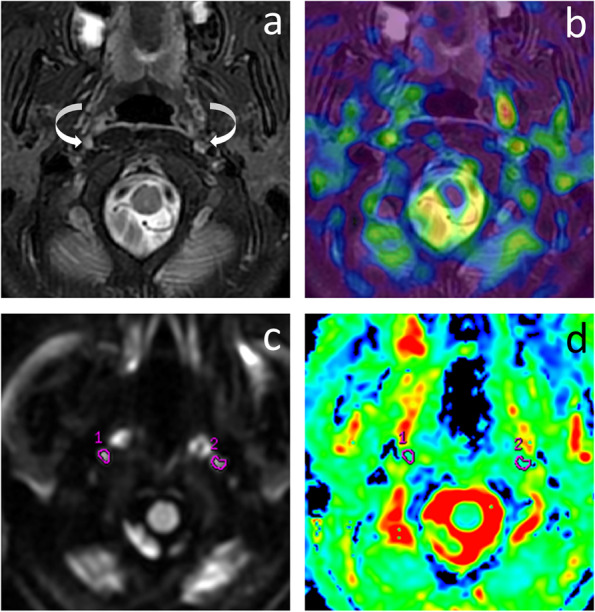
Background: To evaluate the parameters derived from arterial spin labeling (ASL) and multi-b-value diffusion-weighted imaging (DWI) for differentiating retropharyngeal lymph nodes (RLNs) in patients with nasopharyngeal carcinoma (NPC).
Methods: This prospective study included 50 newly diagnosed NPC and 23 healthy control (HC) participants. RLNs of NPC were diagnosed according to the follow-up MRI after radiotherapy. Parameters derived from ASL and multi-b-value DWI, and RLNs axial size on pre-treatment MRI among groups were compared. Receiver operating characteristic curve (ROC) was used to analyze the diagnostic efficiency.
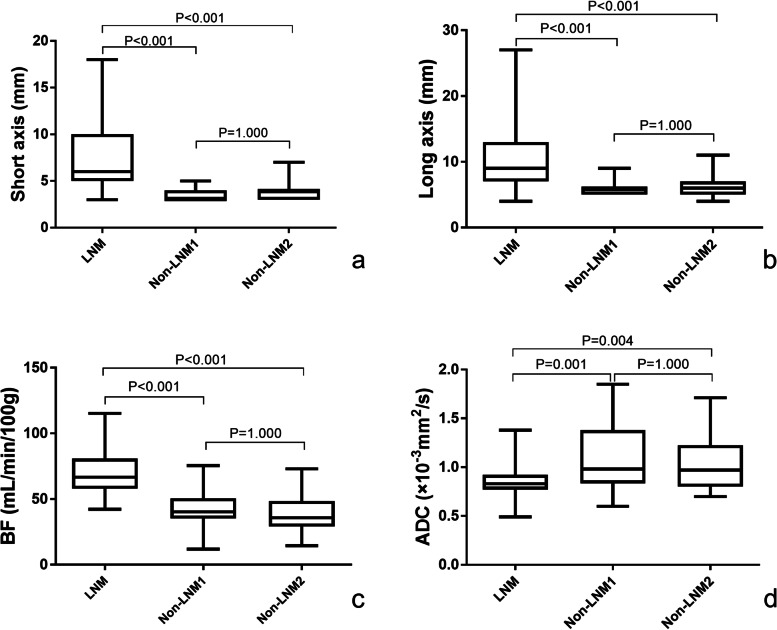
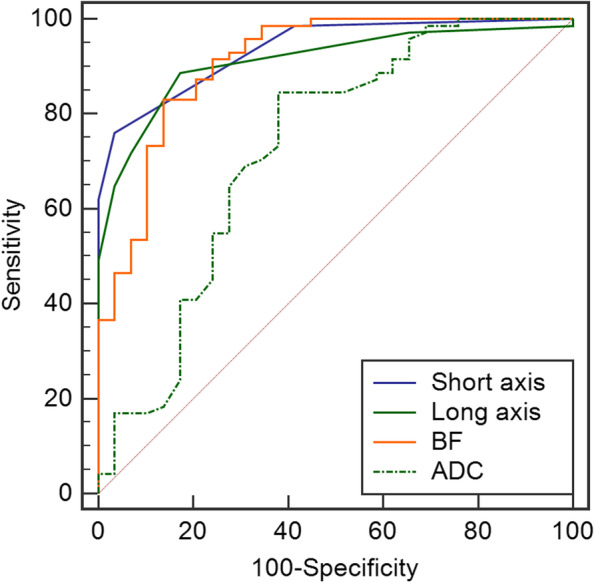
Results: A total of 133 RLNs were collected and divided into a metastatic group (n = 71) and two non-metastatic groups (n = 62, including 29 nodes from NPC and 33 nodes from HC). The axial size, blood flow (BF), and apparent diffusion coefficient (ADC) of RLNs were significantly different between the metastasis and the non-metastasis group. For NPC patients with a short axis < 5 mm or < 6 mm, or long axis < 7 mm, if BF > 54 mL/min/100 g or ADC ≤ 0.95 × 10-3 mm2/s, the RLNs were still considered metastatic. Compared with the index alone, a combination of size and functional parameters could improve the accuracy significantly, except the long axis combined with ADC; especially, combined size with BF exhibited better performance with an accuracy of 91.00-92.00%.
Conclusions: ASL and multi-b-value DWI could help determine the N stage of NPC, while the BF combination with RLNs size may significantly improve the diagnostic efficiency.
Keywords: Diffusion magnetic resonance imaging; Magnetic resonance imaging; Nasopharyngeal neoplasms; Perfusion imaging.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
