

Ultrasound diagnosis of hypertrophic pyloric stenosis - Time to change the criteria
- PMID: 35978726
- PMCID: PMC9351432
- DOI: 10.1002/ajum.12305
Ultrasound diagnosis of hypertrophic pyloric stenosis - Time to change the criteria
Abstract
Introduction: Ultrasound is the examination of choice for the diagnosis of hypertrophic pyloric stenosis (HPS). A correct diagnosis is dependent on the technique and measurement accuracy. However, in the world literature there is a wide range of values suggested for the diagnosis of this condition. The current minimum measurements used to diagnose HPS seem excessively large, and therefore, we set out to redefine these values.
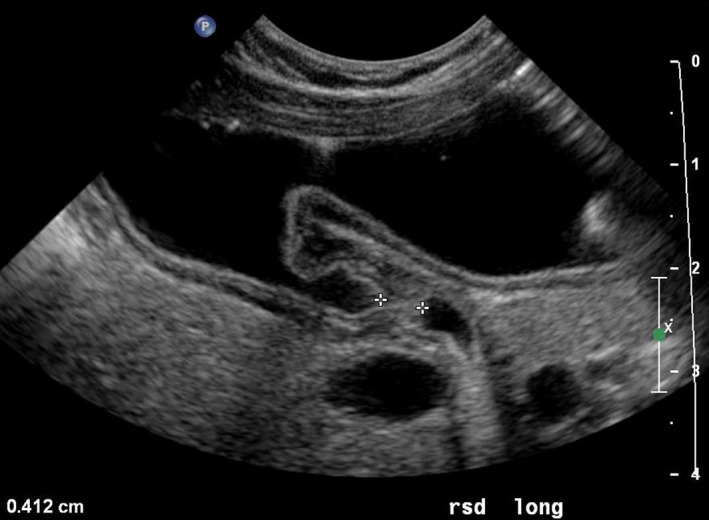
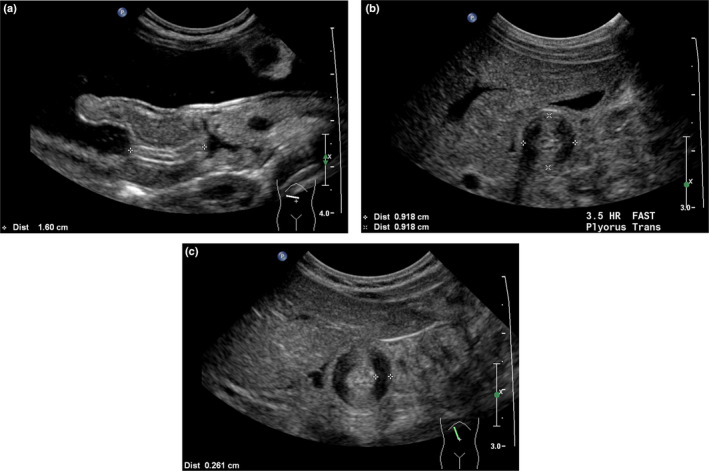
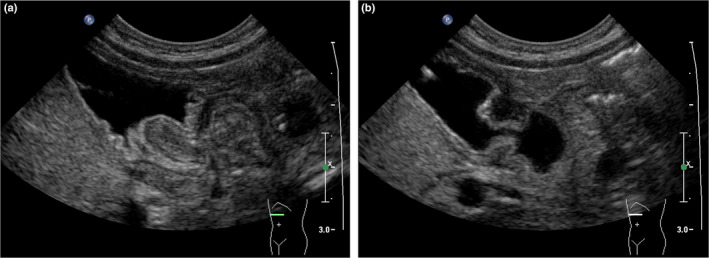
Methods: A retrospective study was performed on 607 patients (615 scans) being investigated for HPS. The length and transverse diameter of the pyloric canal, and thickness of the pyloric muscle were measured. All results were correlated with clinical and surgical findings.
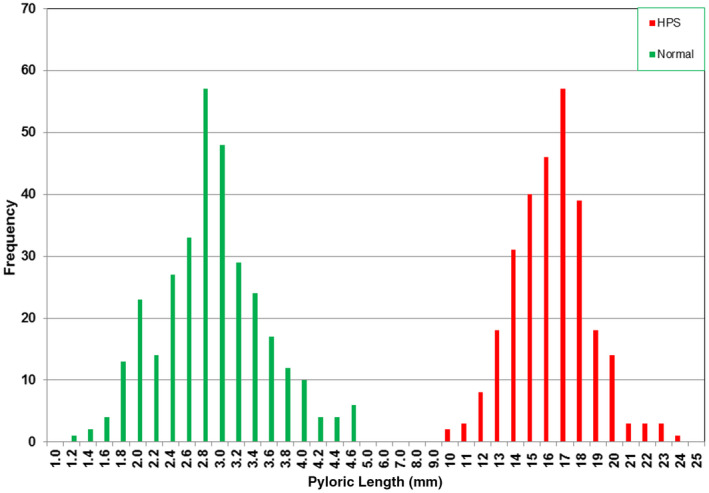
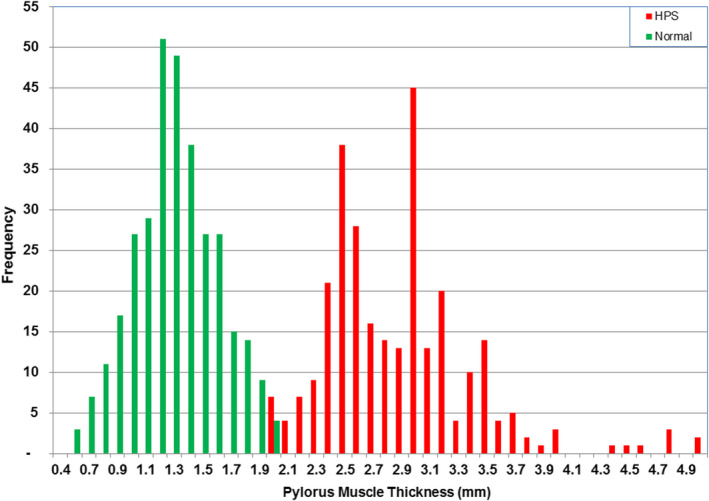
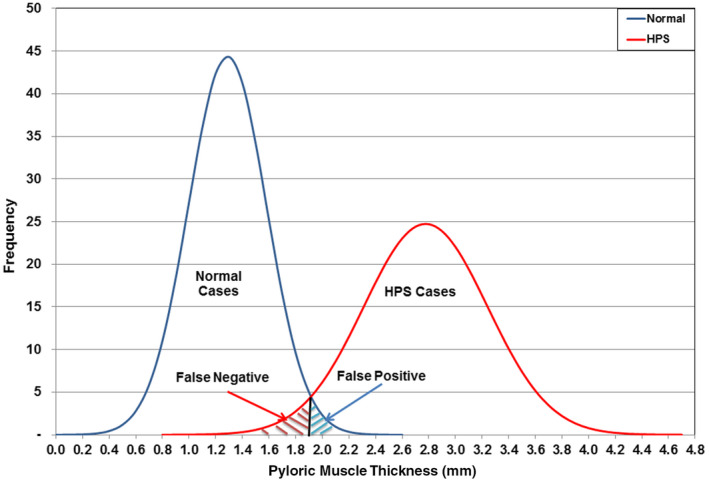
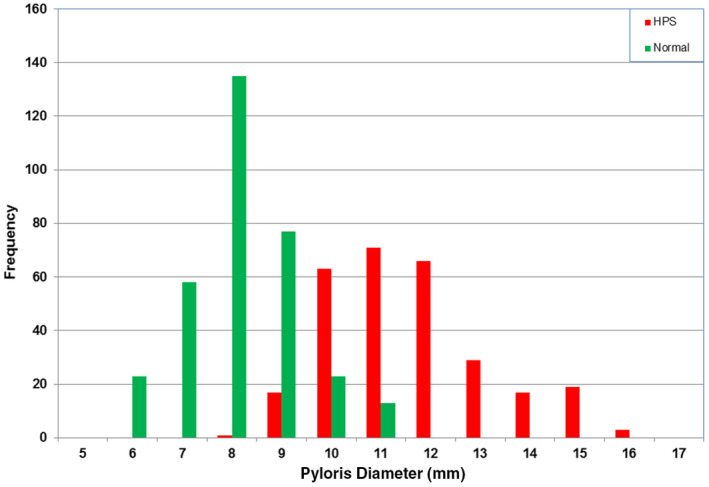
Results: In this study, the muscle thickness in the normal group was <2.0 mm than in HPS infants having a muscle thickness of 2.0-5.0 mm. All the pyloric canal lengths in the normal group were <5.0 mm than in those with HPS having a length of 10.0-24.0 mm. The transverse diameters ranged from 6.0 to 11.0 mm in the normal group compared with those with HPS having a diameter between 8.0 and 16.0 mm.
Conclusions: The current criteria for sonographic diagnosis of HPS should be redefined. The canal length is the single most important discriminator, with a clear separation between normal and abnormal. The commonly used 16.0-mm measurement is too long and should be reduced to 10.0 mm (without the risk of false positives). In many cases, the muscle thickness in those with HPS is as low as 2.0 mm, considerably less than the 3.0 mm that is currently used. The transverse diameter is not a useful discriminator for HPS. The use of current values will delay the diagnosis and timely treatment of this condition.
Keywords: children; hypertrophic pyloric stenosis; ultrasound.
© 2022 Australasian Society for Ultrasound in Medicine.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures

Similar articles
-
The impact of high-frequency transducers on the sonographic measurements of the pyloric muscle thickness in infants.Pediatr Radiol. 2024 May;54(5):737-742. doi: 10.1007/s00247-024-05881-0. Epub 2024 Feb 29. Pediatr Radiol. 2024. PMID: 38418631
-
Hypertrophic pyloric stenosis in newborns younger than 21 days: remodeling the path of surgical intervention.J Pediatr Surg. 2008 Jun;43(6):998-1001. doi: 10.1016/j.jpedsurg.2008.02.022. J Pediatr Surg. 2008. PMID: 18558172
-
[Ultrasonography in the diagnosis of hypertrophic pyloric stenosis and intussusception--emergency conditions in pediatric gastroenterology].Med Pregl. 2007 Sep-Oct;60(9-10):467-72. doi: 10.2298/mpns0710467j. Med Pregl. 2007. PMID: 18265594 Serbian.
-
Diagnostic accuracy of palpation and ultrasonography for diagnosing infantile hypertrophic pyloric stenosis: a systematic review and meta-analysis.Br J Radiol. 2022 Oct 1;95(1139):20211251. doi: 10.1259/bjr.20211251. Epub 2022 Sep 26. Br J Radiol. 2022. PMID: 36043474 Free PMC article.
-
Recurrent hypertrophic pyloric stenosis: Neonatal age and pyloric canal length as risk factors.Pediatr Neonatol. 2025 Jan;66(1):2-6. doi: 10.1016/j.pedneo.2024.10.009. Epub 2024 Nov 29. Pediatr Neonatol. 2025. PMID: 39638742 Review. No abstract available.
Cited by
-
Ultrasound research - Sometimes you win, sometimes you lose.Australas J Ultrasound Med. 2022 Aug 4;25(3):105-106. doi: 10.1002/ajum.12310. eCollection 2022 Aug. Australas J Ultrasound Med. 2022. PMID: 35978729 Free PMC article. No abstract available.
References
-
- Stunden RJ, LeQuesne GW, Little KET. The improved ultrasound diagnosis of hypertrophic pyloric stenosis. Pediatr Radiol 1986; 16: 200–5. - PubMed
-
- Wilson DA, Vanhoutte JJ. The reliable sonographic diagnosis of hypertrophic pyloric stenosis. J Clin Ultrasound 1984; 12: 201–4. - PubMed
-
- Haller JO, Cohen HL. Hypertrophic pyloric stenosis: diagnosis using US. Radiology 1986; 161: 335–9. - PubMed
-
- Blumhagen JD, Maclin L, Krauter D, Rosenbaum DM, Weinberger E. Sonographic diagnosis of hypertrophic pyloric stenosis. AJR 1988; 150: 1367–70. - PubMed
-
- O'Keeffe FN, Stansberry SD, Swischuk LE, Hayden CK Jr. Antropyloric muscle thickness at US in infants: what is normal? Radiology 1991; 178(3): 827–30. - PubMed
LinkOut - more resources
Full Text Sources