

Machine learning for infection risk prediction in postoperative patients with non-mechanical ventilation and intravenous neurotargeted drugs
- PMID: 35979059
- PMCID: PMC9376287
- DOI: 10.3389/fneur.2022.942023
Machine learning for infection risk prediction in postoperative patients with non-mechanical ventilation and intravenous neurotargeted drugs
Abstract
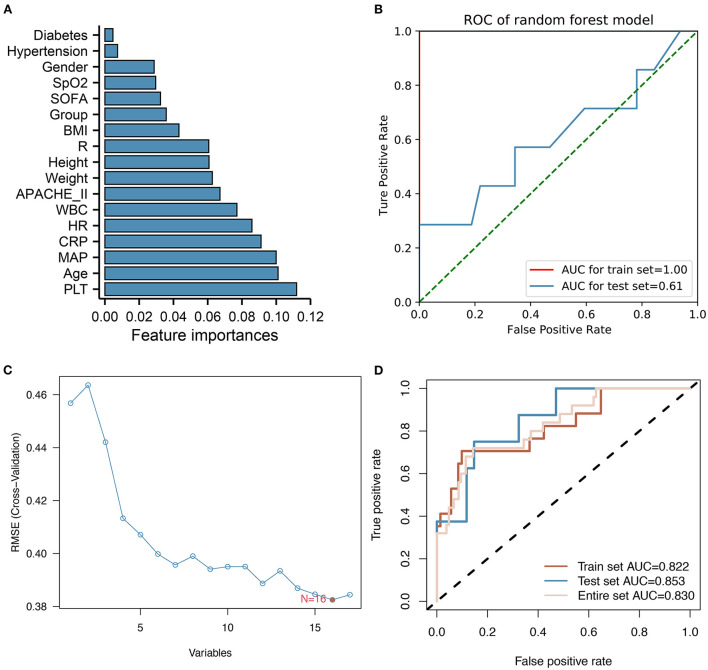
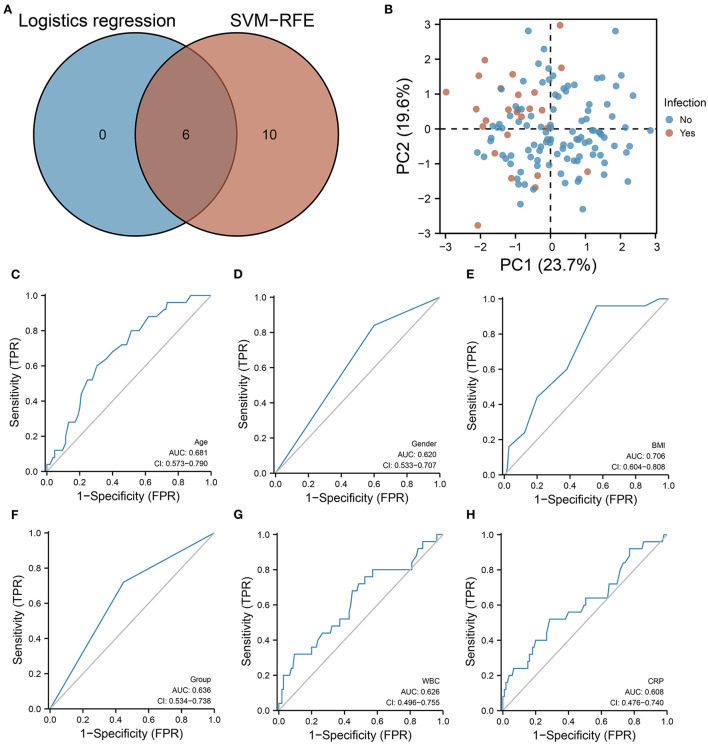
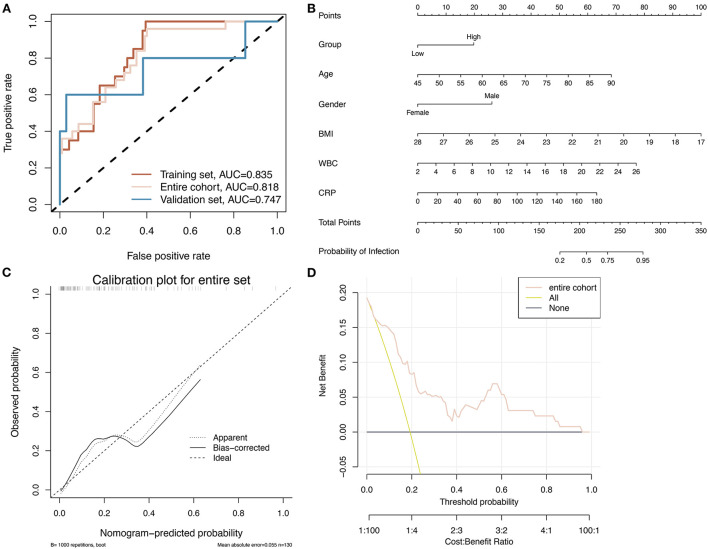
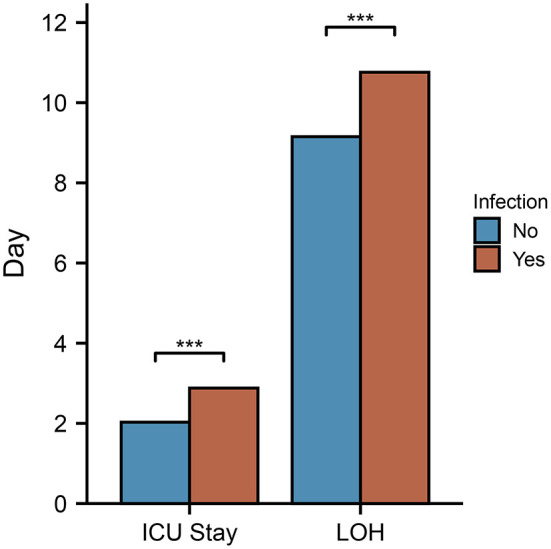
Drug efficacy can be improved by understanding the effects of anesthesia on the neurovascular system. In this study, we used machine learning algorithms to predict the risk of infection in postoperative intensive care unit (ICU) patients who are on non-mechanical ventilation and are receiving hydromorphone analgesia. In this retrospective study, 130 patients were divided into high and low dose groups of hydromorphone analgesic pump patients admitted after surgery. The white blood cells (WBC) count and incidence rate of infection was significantly higher in the high hydromorphone dosage group compared to the low hydromorphone dosage groups (p < 0.05). Furthermore, significant differences in age (P = 0.006), body mass index (BMI) (P = 0.001), WBC count (P = 0.019), C-reactive protein (CRP) (P = 0.038), hydromorphone dosage (P = 0.014), and biological sex (P = 0.024) were seen between the infected and non-infected groups. The infected group also had a longer hospital stay and an extended stay in the intensive care unit compared to the non-infected group. We identified important risk factors for the development of postoperative infections by using machine learning algorithms, including hydromorphone dosage, age, biological sex, BMI, and WBC count. Logistic regression analysis was applied to incorporate these variables to construct infection prediction models and nomograms. The area under curves (AUC) of the model were 0.835, 0.747, and 0.818 in the training group, validation group, and overall pairwise column group, respectively. Therefore, we determined that hydromorphone dosage, age, biological sex, BMI, WBC count, and CRP are significant risk factors in developing postoperative infections.
Keywords: anesthesia; hydromorphone; infection; machine learning; neurovascular; post-surgical ICU.
Copyright © 2022 Du, Shi, Yang and Wu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Effects of patient-controlled analgesia with hydromorphone or sufentanil on postoperative pulmonary complications in patients undergoing thoracic surgery: a quasi-experimental study.BMC Anesthesiol. 2018 Dec 19;18(1):192. doi: 10.1186/s12871-018-0657-7. BMC Anesthesiol. 2018. PMID: 30567490 Free PMC article. Clinical Trial.
-
[Diagnosis value of serum infection index for early infection of patients undergoing posterior cervical expansive open-door laminoplasty].Zhongguo Gu Shang. 2019 Oct 25;32(10):892-897. doi: 10.3969/j.issn.1003-0034.2019.10.004. Zhongguo Gu Shang. 2019. PMID: 32512957 Chinese.
-
[Risk factors for death in elderly patients admitted to intensive care unit after elective abdominal surgery: a consecutive 5-year retrospective study].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021 Dec;33(12):1453-1458. doi: 10.3760/cma.j.cn121430-20210804-00118. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021. PMID: 35131012 Chinese.
-
Analgosedation: The Use of Fentanyl Compared to Hydromorphone.J Crit Care Med (Targu Mures). 2021 Aug 5;7(3):192-198. doi: 10.2478/jccm-2021-0026. eCollection 2021 Jul. J Crit Care Med (Targu Mures). 2021. PMID: 34722922 Free PMC article.
-
Effectiveness of dexmedetomidine versus propofol on extubation times, length of stay and mortality rates in adult cardiac surgery patients: a systematic review and meta-analysis.JBI Database System Rev Implement Rep. 2018 May;16(5):1220-1239. doi: 10.11124/JBISRIR-2017-003488. JBI Database System Rev Implement Rep. 2018. PMID: 29762314
Cited by
-
Prediction of Complications and Prognostication in Perioperative Medicine: A Systematic Review and PROBAST Assessment of Machine Learning Tools.Anesthesiology. 2024 Jan 1;140(1):85-101. doi: 10.1097/ALN.0000000000004764. Anesthesiology. 2024. PMID: 37944114 Free PMC article.
-
Predictors of cognitive impairment in patients undergoing ileostomy for colorectal cancer: a retrospective analysis.PeerJ. 2023 Jun 5;11:e15405. doi: 10.7717/peerj.15405. eCollection 2023. PeerJ. 2023. PMID: 37304889 Free PMC article. Clinical Trial.
References
-
- Chanques G, Sebbane M, Barbotte E, Viel E, Eledjam J-J, Jaber S, et al. . Prospective study of pain at rest: incidence and characteristics of an unrecognized symptom in surgical and trauma versus medical intensive care unit patients. Anesthesiology. (2007) 107:858–60. 10.1097/01.anes.0000287211.98642.51 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous