

Combined thoracic paravertebral block and interscalene brachial plexus block for modified radical mastectomy: A case report
- PMID: 35979098
- PMCID: PMC9258351
- DOI: 10.12998/wjcc.v10.i17.5741
Combined thoracic paravertebral block and interscalene brachial plexus block for modified radical mastectomy: A case report
Abstract
Background: Modified radical mastectomy (MRM) is the most common surgical treatment for breast cancer. General anesthesia poses a challenge in fragile MRM patients, including cardiovascular instability, insufficient postoperative pain control, nausea and vomiting. Thoracic paravertebral block (TPVB) is adequate for simple mastectomy, but its combination with interscalene brachial plexus block (IBPB) has not yet been proved to be an effective anesthesia method for MRM.
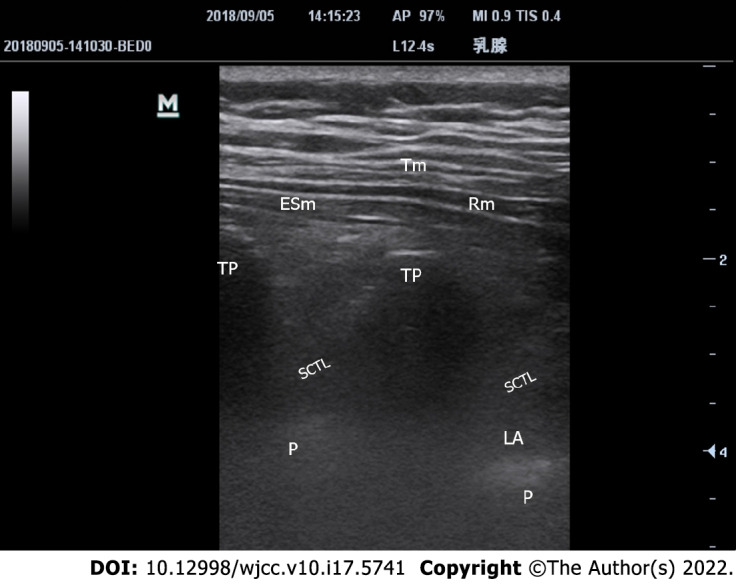
Case summary: We describe our experience of anesthesia and pain management in 10 patients with multiple comorbidities. An ultrasound-guided TPVB was placed at T2-T3 and T5-T6, and combined with IBPB, with administration of 10, 15 and 5 mL of 0.5% ropivacaine, respectively. A satisfactory anesthetic effect was proved by the absence of ipsilateral tactile sensation within 30 min. Propofol 3 mg/kg/h and oxygen supplementation via a nasal cannula were administered during surgery. None of the patients required additional narcotics, vasopressors, or conversion to general anesthesia. The maximum pain score was 2 on an 11-point numerical rating scale. Two patients required one dose of celecoxib 8 h postoperatively and none reported nausea or emesis.
Conclusion: This case series demonstrated that combined two-site TPVB and small-volume IBPB with sedation can be used as an alternative anesthetic modality for MRM, providing good postoperative analgesia.
Keywords: Brachial plexus block; Case report; Modified radical mastectomy; Paravertebral block; Sedation.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflict of interest.
Figures
References
-
- DeSantis CE, Ma J, Gaudet MM, Newman LA, Miller KD, Goding Sauer A, Jemal A, Siegel RL. Breast cancer statistics, 2019. CA Cancer J Clin. 2019;69:438–451. - PubMed
-
- Jones C, Lancaster R. Evolution of Operative Technique for Mastectomy. Surg Clin North Am. 2018;98:835–844. - PubMed
-
- Shirakami G, Teratani Y, Segawa H, Matsuura S, Shichino T, Fukuda K. Omission of fentanyl during sevoflurane anesthesia decreases the incidences of postoperative nausea and vomiting and accelerates postanesthesia recovery in major breast cancer surgery. J Anesth. 2006;20:188–195. - PubMed
-
- Sessler DI, Pei L, Huang Y, Fleischmann E, Marhofer P, Kurz A, Mayers DB, Meyer-Treschan TA, Grady M, Tan EY, Ayad S, Mascha EJ, Buggy DJ Breast Cancer Recurrence Collaboration. Recurrence of breast cancer after regional or general anaesthesia: a randomised controlled trial. Lancet. 2019;394:1807–1815. - PubMed
-
- Malik OS, Brovman EY, Urman RD. The Use of Regional or Local Anesthesia for Carotid Endarterectomies May Reduce Blood Loss and Pulmonary Complications. J Cardiothorac Vasc Anesth. 2019;33:935–942. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
