

Usefulness of serum C-reactive protein and calprotectin for the early detection of colorectal anastomotic leakage: A prospective observational study
- PMID: 35979163
- PMCID: PMC9260864
- DOI: 10.3748/wjg.v28.i24.2758
Usefulness of serum C-reactive protein and calprotectin for the early detection of colorectal anastomotic leakage: A prospective observational study
Abstract
Background: Colorectal anastomotic leakage (CAL) is one of the most dreaded complications after colorectal surgery, with an incidence that can be as high as 27%. This event is associated with increased morbidity and mortality; therefore, its early diagnosis is crucial to reduce clinical consequences and costs. Some biomarkers have been suggested as laboratory tools for the diagnosis of CAL.
Aim: To assess the usefulness of plasma C-reactive protein (CRP) and calprotectin (CLP) as early predictors of CAL.
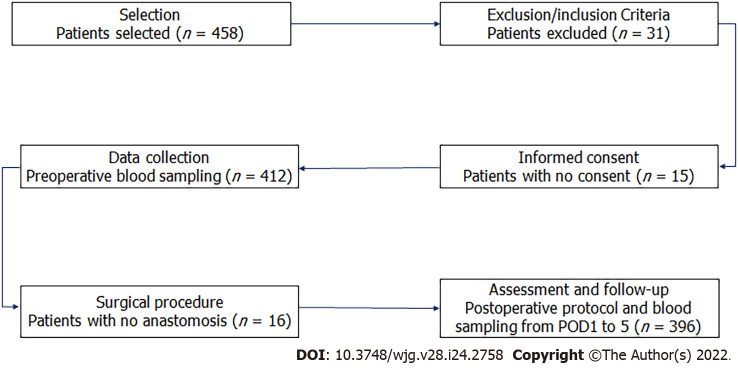
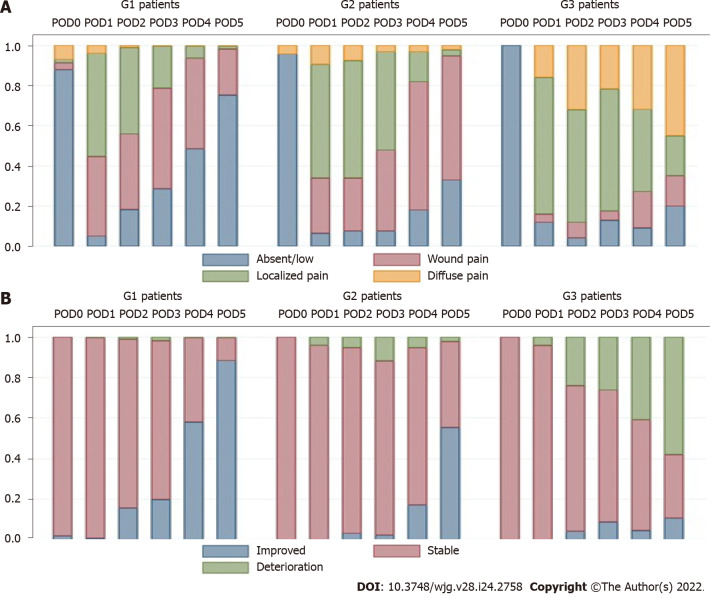
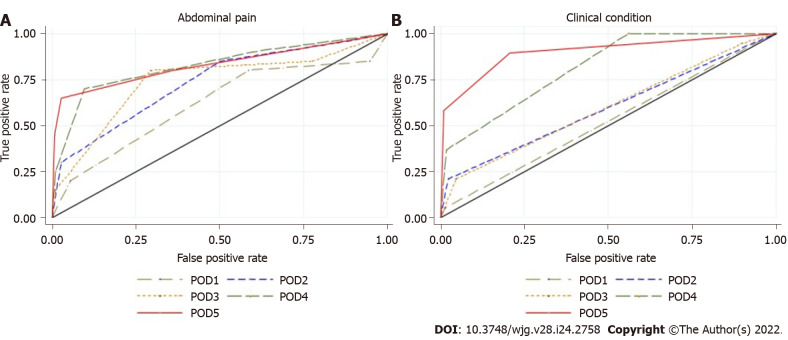
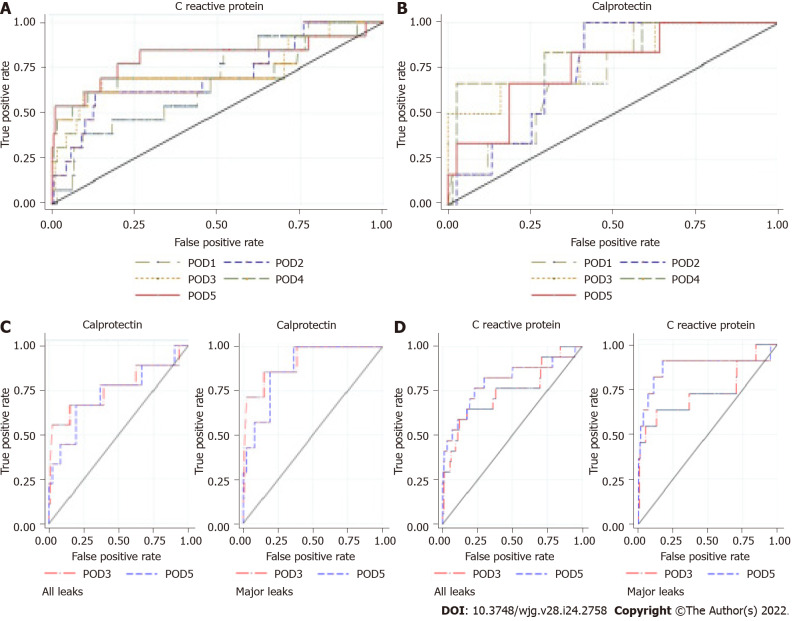
Methods: A prospective monocentric observational study was conducted including patients who underwent colorectal resection with anastomosis, from March 2017 to August 2019. Patients were divided into three groups: G1 - no complications; G2 - complications not related to CAL; and G3 - CAL. Five biomarkers were measured and analyzed in the first 5 postoperative days (PODs), namely white blood cell (WBC) count, eosinophil cell count (ECC), CRP, CLP, and procalcitonin (PCT). Clinical criteria, such as abdominal pain and clinical condition, were also assessed. The correlation between biomarkers and CAL was evaluated. Receiver operating characteristic (ROC) curve analysis was used to compare the accuracy of these biomarkers as predictors of CAL, and the area under the ROC curve (AUROC), specificity, sensitivity, positive predictive value, and negative predictive value (NPV) during this period were estimated.
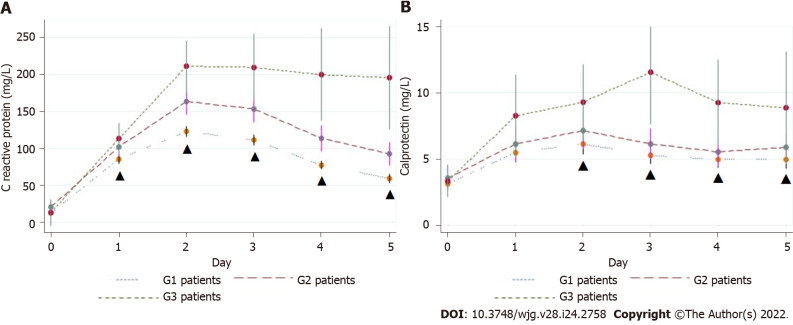
Results: In total, 25 of 396 patients developed CAL (6.3%), and the mean time for this diagnosis was 9.0 ± 6.8 d. Some operative characteristics, such as surgical approach, blood loss, intraoperative complications, and duration of the procedure, were notably related to the development of CAL. The length of hospital stay was markedly higher in the group that developed CAL compared with the group with complications other than CAL and the group with no complications (median of 21 d vs 13 d and 7 d respectively; P < 0.001). For abdominal pain, the best predictive performance was on POD4 and POD5, with the largest AUROC of 0.84 on POD4. Worsening of the clinical condition was associated with the diagnosis of CAL, presenting a higher predictive effect on POD5, with an AUROC of 0.9. WBC and ECC showed better predictive effects on POD5 (AUROC = 0.62 and 0.7, respectively). Those markers also presented a high NPV (94%-98%). PCT had the best predictive effect on POD5 (AUROC = 0.61), although it presented low accuracy. However, this biomarker revealed a high NPV on POD3, POD4, and POD5 (96%, 95%, and 96%, respectively). The mean CRP value on POD5 was significantly higher in the group that developed CAL compared with the group without complications (195.5 ± 139.9 mg/L vs 59.5 ± 43.4 mg/L; P < 0.00001). On POD5, CRP had a NPV of 98%. The mean CLP value on POD3 was significantly higher in G3 compared with G1 (5.26 ± 3.58 μg/mL vs 11.52 ± 6.81 μg/mL; P < 0.00005). On POD3, the combination of CLP and CRP values showed a high diagnostic accuracy (AUROC = 0.82), providing a 5.2 d reduction in the time to CAL diagnosis.
Conclusion: CRP and CLP are moderate predictors of CAL. However, the combination of these biomarkers presents an increased diagnostic accuracy, potentially decreasing the time to CAL diagnosis.
Keywords: Anastomotic leakage; Biomarkers; C-reactive protein; Calprotectin; Colorectal; Surgery.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Procalcitonin and C-reactive protein as early markers of anastomotic leak after laparoscopic colorectal surgery within an enhanced recovery after surgery (ERAS) program.Surg Endosc. 2018 Sep;32(9):4003-4010. doi: 10.1007/s00464-018-6144-x. Epub 2018 Mar 8. Surg Endosc. 2018. PMID: 29520440
-
C-reactive Protein and Procalcitonin Levels to Predict Anastomotic Leak After Colorectal Surgery: Systematic Review and Meta-analysis.J Gastrointest Surg. 2023 Jan;27(1):166-179. doi: 10.1007/s11605-022-05473-z. Epub 2022 Sep 29. J Gastrointest Surg. 2023. PMID: 36175720
-
Development of a warning score for early detection of colorectal anastomotic leakage: Hype or hope?World J Gastrointest Surg. 2022 Nov 27;14(11):1297-1309. doi: 10.4240/wjgs.v14.i11.1297. World J Gastrointest Surg. 2022. PMID: 36504511 Free PMC article.
-
Anastomotic leakage after elective colorectal surgery: a prospective multicentre observational study on use of the Dutch leakage score, serum procalcitonin and serum C-reactive protein for diagnosis.BJS Open. 2020 Jun;4(3):499-507. doi: 10.1002/bjs5.50269. Epub 2020 Mar 5. BJS Open. 2020. PMID: 32134216 Free PMC article.
-
Use of C-reactive protein for the early prediction of anastomotic leak after esophagectomy: Systematic review and Bayesian meta-analysis.PLoS One. 2018 Dec 17;13(12):e0209272. doi: 10.1371/journal.pone.0209272. eCollection 2018. PLoS One. 2018. PMID: 30557392 Free PMC article.
Cited by
-
Predictive Value of C-Reactive Protein for Infectious Complications After Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy: A Single-Center Prospective Study.Ann Surg Oncol. 2024 Dec;31(13):8538-8548. doi: 10.1245/s10434-024-15986-3. Epub 2024 Aug 12. Ann Surg Oncol. 2024. PMID: 39134911
-
C-reactive protein and digestive pathologies: A narrative review for daily clinical use.J Res Med Sci. 2025 Feb 28;30:10. doi: 10.4103/jrms.jrms_537_23. eCollection 2025. J Res Med Sci. 2025. PMID: 40200962 Free PMC article. Review.
-
Elevated drain fluid calprotectin as a predictor of early anastomotic leakage in colorectal surgery.World J Surg Oncol. 2025 Jun 23;23(1):247. doi: 10.1186/s12957-025-03899-8. World J Surg Oncol. 2025. PMID: 40551176 Free PMC article.
-
Procalcitonin as an Early Marker of Colorectal Anastomotic Leakage in Postoperative Colorectal Cancer Patients: A Systematic Review and Meta-Analysis.Cureus. 2024 Oct 1;16(10):e70647. doi: 10.7759/cureus.70647. eCollection 2024 Oct. Cureus. 2024. PMID: 39483587 Free PMC article. Review.
-
Feasibility and safety of specimen extraction via an enlarged (U-Plus) skin bridge loop ileostomy: a single-center retrospective comparative study.Front Oncol. 2023 Nov 8;13:1273499. doi: 10.3389/fonc.2023.1273499. eCollection 2023. Front Oncol. 2023. PMID: 38023201 Free PMC article.
References
-
- Boccola MA, Buettner PG, Rozen WM, Siu SK, Stevenson AR, Stitz R, Ho YH. Risk factors and outcomes for anastomotic leakage in colorectal surgery: a single-institution analysis of 1576 patients. World J Surg. 2011;35:186–195. - PubMed
-
- Trencheva K, Morrissey KP, Wells M, Mancuso CA, Lee SW, Sonoda T, Michelassi F, Charlson ME, Milsom JW. Identifying important predictors for anastomotic leak after colon and rectal resection: prospective study on 616 patients. Ann Surg. 2013;257:108–113. - PubMed
-
- Pommergaard HC, Gessler B, Burcharth J, Angenete E, Haglind E, Rosenberg J. Preoperative risk factors for anastomotic leakage after resection for colorectal cancer: a systematic review and meta-analysis. Colorectal Dis. 2014;16:662–671. - PubMed
-
- McDermott FD, Heeney A, Kelly ME, Steele RJ, Carlson GL, Winter DC. Systematic review of preoperative, intraoperative and postoperative risk factors for colorectal anastomotic leaks. Br J Surg. 2015;102:462–479. - PubMed
-
- Smith SR, Pockney P, Holmes R, Doig F, Attia J, Holliday E, Carroll R, Draganic B. Biomarkers and anastomotic leakage in colorectal surgery: C-reactive protein trajectory is the gold standard. ANZ J Surg. 2018;88:440–444. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
