

Lymphogranuloma Venereum-Associated Proctitis Mimicking a Malignant Rectal Neoplasia: Searching for Diagnosis
- PMID: 35979244
- PMCID: PMC9274944
- DOI: 10.1159/000516011
Lymphogranuloma Venereum-Associated Proctitis Mimicking a Malignant Rectal Neoplasia: Searching for Diagnosis
Abstract
Background: Chlamydia trachomatis-lymphogranuloma venereum (LGV) is a sexually transmitted infection (STI) and an uncommon cause of proctitis. The diagnosis requires a high index of clinical suspicion, since the clinical, imaging, endoscopic, and histological findings can mimic multiple benign or malignant conditions like inflammatory bowel disease and rectal neoplasms.
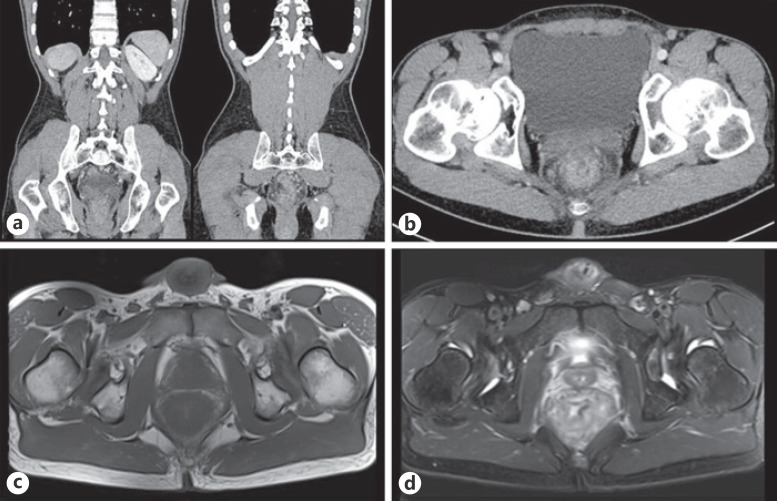
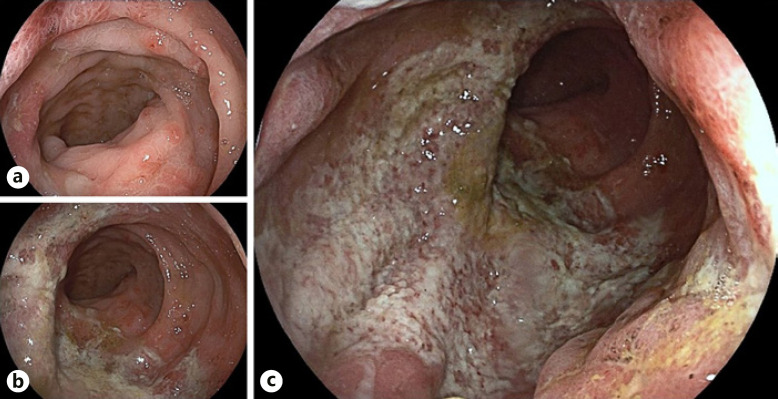
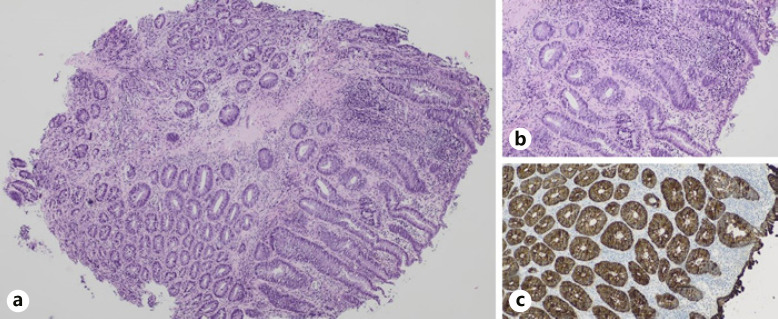
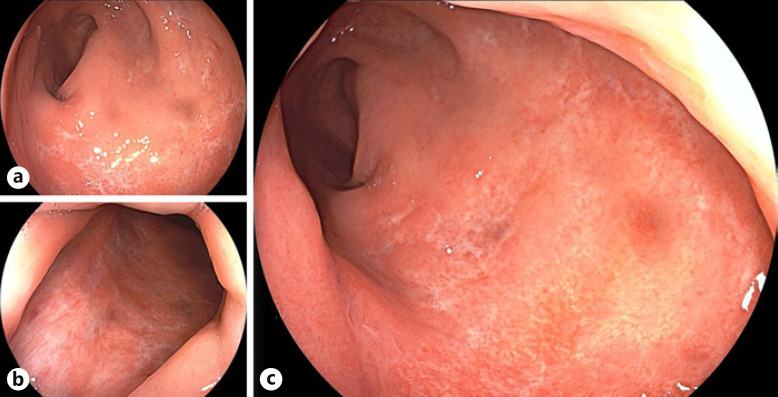
Case presentation: We present the case of a 48-year-old Caucasian male with no significant previous medical history who was admitted due to the suspicion of a rectal neoplasia. He underwent an abdominopelvic computed tomography (CT) scan and pelvic magnetic resonance imaging (MRI) before admission due to complaints of anorectal pain, hematochezia, and constipation over the previous 2 weeks. The examination revealed a circumferential rectal wall thickening, infiltration of the perirectal fat and invasion of the mesorectal fascia, associated with perirectal fat lymphadenopathy. A radiological diagnosis of a rectal malignant neoplasia staged as T4N2MX was stated. Digital rectal examination identified a circumferential rectal tumor. Rectosigmoidoscopy showed an extensive and circumferential ulceration of the rectal mucosa, with elevated geographical borders, exudate, and aphthoid erosions at the proximal limit of the endoscopic mucosal ulceration. Biopsy specimens revealed acute ulcerative proctitis with lymphoplasmocytic inflammatory infiltrate but no evidence of dysplasia or malignancy. A STI screening was positive for HIV-1 (CD4+ 251/mm3; N = 700-1,100) and C. trachomatis, with an elevated IgA-specific antibody titer (52.000; N < 5.0), suggesting LGV disease. The diagnosis was confirmed by the identification of C. trachomatis DNA on rectal swab. Other infectious causes of acute proctitis were excluded. When faced with these results, the patient ended up mentioning that he had unprotected anal sex with men. He started treatment with doxycycline 100 mg twice a day for 21 days, with a drastic improvement. Rectosigmoidoscopy was repeated and showed clear signs of progressive resolution of the ulcerative proctitis.
Discussion: LGV-associated proctitis, often undervalued, is a reemerging disease which should always be considered a benign cause of rectal mass, in order to avoid delay in diagnosis and development of complications. Diagnosis becomes more challenging in patients with unknown HIV status. A detailed clinical history, including sexual behaviors, is a vital step to achieve the final diagnosis.
Introdução: A infeção por Chlamydia trachomatis-linfogranuloma venéreo (LGV) é uma doença sexualmente transmissível (DST), sendo uma causa incomum de proctite. O diagnóstico exige um elevado grau de suspeição, dado que os achados clínicos, radiológicos, endoscópicos e histológicos podem mimetizar múltiplas condições benignas ou malignas, como a doença inflamatória intestinal e as neoplasias retais.
Caso clínico: Apresentamos o caso de um homem de 48 anos, caucasiano, sem antecedentes relevantes, admitido por suspeita de neoplasia retal. Por queixas de dor anorretal, hematoquézias e obstipação com 2 semanas de evolução, realizou uma tomografia computadorizada abdominopélvica e uma ressonância magnética pélvica, que revelaram espessamento retal circunferencial, infiltração da gordura periretal e invasão da fáscia mesoretal, associados a linfadenopatias locais, sugestivos de malignidade retal (T4N2MX). O toque retal identificou uma tumoração retal circunferencial.A retosigmoidoscopia mostrou mucosa retal com ulceração extensa e circunferencial, bordos geográficos elevados, exsudado e erosões aftóides no limite proximal da ulceração mucosa. As biópsias revelaram proctite ulcerada aguda com infiltrado linfoplasmocitário difuso, sem displasia ou neoplasia. O screening de DST foi positivo para VIH-1 (CD4+ 251/mm3; N: 700–1100) e título elevado de IgA para C. trachomatis (52 000; N< 5), sugerindo LGV. O diagnóstico foi confirmado pela identificação do DNA de C. trachomatis em zaragatoa retal. Outras causas infecciosas de proctite aguda foram excluídas. Perante estes resultados, o doente acabou por mencionar que tinha tido relações homossexuais anais desprotegidas. Iniciou doxiciclina (100 mg duas vezes por dia, por 21 dias) com melhoria sintomática drástica. Repetiu retosigmoidoscopia, com sinais de proctite ulcerada em resolução.
Discussão: A proctite por LGV, frequentemente desvalorizada, é uma doença re-emergente, que deve ser sempre equacionada como causa benigna de massa retal, de modo a evitar o atraso diagnóstico e o desenvolvimento de complicações. O diagnóstico torna-se mais desafiante em doentes com status VIH desconhecido. A história clínica detalhada, incluindo comportamentos sexuais de risco, é fundamental para o diagnóstico.
Keywords: Chlamydia trachomatis; Lymphogranuloma venereum; Proctitis; Rectal cancer.
Copyright © 2021 by Sociedade Portuguesa de Gastrenterologia Published by S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Rectal Lymphogranuloma Venereum Mass Mimicking Colorectal Cancer.Cureus. 2025 Feb 4;17(2):e78516. doi: 10.7759/cureus.78516. eCollection 2025 Feb. Cureus. 2025. PMID: 40062065 Free PMC article.
-
Lymphogranuloma Venereum Mimicking Locally Metastatic Rectal Cancer in an HIV-Negative Man.Cureus. 2021 Dec 6;13(12):e20216. doi: 10.7759/cureus.20216. eCollection 2021 Dec. Cureus. 2021. PMID: 35004036 Free PMC article.
-
Anorectal Lymphogranuloma Venereum in Madrid: A Persistent Emerging Problem in Men Who Have Sex With Men.Sex Transm Dis. 2016 Jul;43(7):414-9. doi: 10.1097/OLQ.0000000000000459. Sex Transm Dis. 2016. PMID: 27322040
-
Lymphogranuloma Venereum 2015: Clinical Presentation, Diagnosis, and Treatment.Clin Infect Dis. 2015 Dec 15;61 Suppl 8:S865-73. doi: 10.1093/cid/civ756. Clin Infect Dis. 2015. PMID: 26602624 Review.
-
Inflammatory bowel disease versus Chlamydia trachomatis infection: a case report and revision of the literature.Eur J Gastroenterol Hepatol. 2020 Mar;32(3):454-457. doi: 10.1097/MEG.0000000000001605. Eur J Gastroenterol Hepatol. 2020. PMID: 31851086 Review.
Cited by
-
[Persistent proctitis and anorectal ulcer].Chirurgie (Heidelb). 2023 Nov;94(11):951-953. doi: 10.1007/s00104-023-01961-3. Epub 2023 Sep 4. Chirurgie (Heidelb). 2023. PMID: 37665361 Free PMC article. German. No abstract available.
-
Case series of perianal and pelvic MRI imaging findings in monkeypox.BJR Case Rep. 2022 Sep 26;9(4):20220109. doi: 10.1259/bjrcr.20220109. eCollection 2023 Aug. BJR Case Rep. 2022. PMID: 37576001 Free PMC article.
-
Challenges in Diagnostic of the Ulcerative Rectitis by Lymphogranuloma venereum in Chlamydia trachomatis Infection and AIDS.Cureus. 2023 Feb 24;15(2):e35420. doi: 10.7759/cureus.35420. eCollection 2023 Feb. Cureus. 2023. PMID: 36987466 Free PMC article.
-
Rectal Lymphogranuloma Venereum Mass Mimicking Colorectal Cancer.Cureus. 2025 Feb 4;17(2):e78516. doi: 10.7759/cureus.78516. eCollection 2025 Feb. Cureus. 2025. PMID: 40062065 Free PMC article.
-
Separating Infectious Proctitis from Inflammatory Bowel Disease-A Common Clinical Conundrum.Microorganisms. 2024 Nov 22;12(12):2395. doi: 10.3390/microorganisms12122395. Microorganisms. 2024. PMID: 39770599 Free PMC article. Review.
References
-
- de Vries HJ, Zingoni A, White JA, Ross JD, Kreuter A. 2013 European Guideline on the management of proctitis, proctocolitis and enteritis caused by sexually transmissible pathogens. Int J STD AIDS. 2014 Jun;25((7)):465–74. - PubMed
-
- Levy I, Gefen-Halevi S, Nissan I, Keller N, Pilo S, Wieder-Finesod A, et al. Delayed diagnosis of colorectal sexually transmitted diseases due to their resemblance to inflammatory bowel diseases. Int J Infect Dis. 2018 Oct;75:34–8. - PubMed
-
- Neri B, Stingone C, Romeo S, Sena G, Gesuale C, Compagno M, et al. Inflammatory bowel disease versus Chlamydia trachomatis infection: a case report and revision of the literature. Eur J Gastroenterol Hepatol. 2020 Mar;32((3)):454–7. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
