

Isolated cryptococcal osteomyelitis of the ulna in an immunocompetent patient: A case report
- PMID: 35979300
- PMCID: PMC9294900
- DOI: 10.12998/wjcc.v10.i19.6617
Isolated cryptococcal osteomyelitis of the ulna in an immunocompetent patient: A case report
Abstract
Background: Cryptococcal osteomyelitis is a bone infection caused by cryptococcus. As an opportunistic infection, bone cryptococcosis usually occurs in patients with immunodeficiency diseases or in those undergoing immunosuppressive therapy and often displays characteristics of disseminated disease. Isolated cryptococcal osteomyelitis is extremely unusual in immunocompetent person. The pathogenic fungus often invades vertebrae, femur, tibia, rib, clavicle, pelvis, and humerus, but the ulna is a rare target.
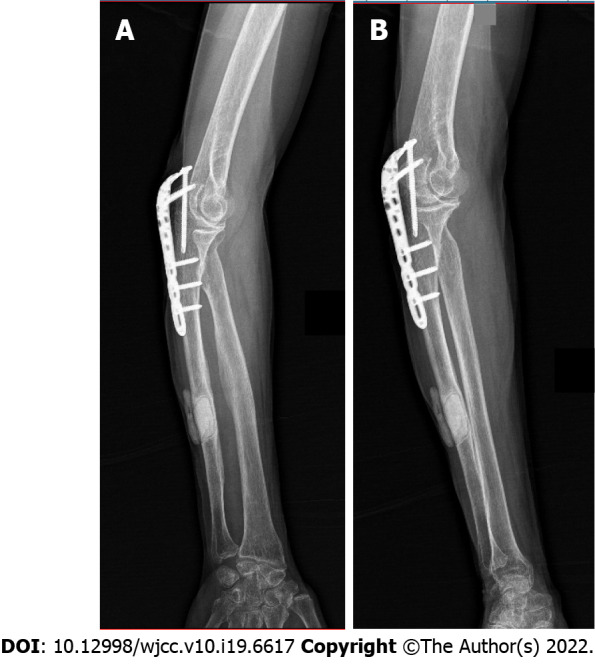
Case summary: A 79-year-old woman complaining of chronic pain, skin ulceration and a sinus on her right forearm was admitted, and soon after was diagnosed with cryptococcal osteomyelitis in the right ulna. Unexpectedly, she was also found to have apparently normal immunity. After treatment with antifungal therapy combined with surgery debridement, the patient's osteomyelitis healed with a satisfactory outcome.
Conclusion: Although rare, cryptococcal osteomyelitis should be considered in the differential diagnosis of osteolytic lesions even in immunocompetent patients, and good outcomes can be expected if early definitive diagnosis and etiological treatment are established.
Keywords: Case report; Cryptococcus neoformans; Immunocompetence; Isolated lesions; Osteomyelitis; Ulna.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflict of interest.
Figures








Similar articles
-
Isolated cryptococcal osteomyelitis of the sacrum in an immunocompetent patient: a case report and literature review.BMC Infect Dis. 2023 Feb 24;23(1):116. doi: 10.1186/s12879-023-08066-6. BMC Infect Dis. 2023. PMID: 36829132 Free PMC article. Review.
-
Isolated cryptococcal osteomyelitis in immunocompetent patient.J Indian Med Assoc. 2011 Aug;109(8):592, 594. J Indian Med Assoc. 2011. PMID: 22315871
-
Isolated cryptococcal osteomyelitis in an immune-competent host: a case report.Int J Infect Dis. 2013 Dec;17(12):e1229-31. doi: 10.1016/j.ijid.2013.04.013. Epub 2013 Jun 15. Int J Infect Dis. 2013. PMID: 23777597
-
Isolated cryptococcal thoracic empyema with osteomyelitis of the rib in an immunocompetent host.J Infect. 2005 Oct;51(3):e117-9. doi: 10.1016/j.jinf.2004.10.011. Epub 2004 Nov 23. J Infect. 2005. PMID: 16230188
-
Disseminated Cryptococcosis in An Immunocompetent Host Presenting As Osteomyelitis and Leading to Adrenal Insufficiency.Am J Med Sci. 2022 Jan;363(1):75-79. doi: 10.1016/j.amjms.2020.12.007. Epub 2020 Dec 13. Am J Med Sci. 2022. PMID: 35033296 Review.
Cited by
-
Isolated cryptococcal osteomyelitis of the sacrum in an immunocompetent patient: a case report and literature review.BMC Infect Dis. 2023 Feb 24;23(1):116. doi: 10.1186/s12879-023-08066-6. BMC Infect Dis. 2023. PMID: 36829132 Free PMC article. Review.
-
Cryptococcus neoformans osteomyelitis of the tibia: a case report and review of the literature.J Med Case Rep. 2023 May 7;17(1):188. doi: 10.1186/s13256-023-03925-x. J Med Case Rep. 2023. PMID: 37149631 Free PMC article. Review.
-
Pubis Cryptococcal Osteomyelitis in an Immunocompetent Patient: A Case Report and Recent Literature Review.Infect Drug Resist. 2022 Dec 14;15:7369-7375. doi: 10.2147/IDR.S390881. eCollection 2022. Infect Drug Resist. 2022. PMID: 36540104 Free PMC article.
-
Cryptococcus neoformans osteomyelitis of the radius treatment with antifungal calcium sulphate: A case report and literature review.Heliyon. 2024 Sep 14;10(19):e37514. doi: 10.1016/j.heliyon.2024.e37514. eCollection 2024 Oct 15. Heliyon. 2024. PMID: 39403459 Free PMC article.
-
Disseminated Cryptococcus neoformans infection involving multiple bones and lung in an immunocompetent patient: a case report.BMC Infect Dis. 2024 Apr 12;24(1):397. doi: 10.1186/s12879-024-09264-6. BMC Infect Dis. 2024. PMID: 38609851 Free PMC article.
References
-
- Jain K Mruthyunjaya, Ravishankar R. Cryptococcal abscess and osteomyelitis of the proximal phalanx of the hand. Indian J Pathol Microbiol. 2011;54:216–218. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
