

Giant retroperitoneal liposarcoma treated with radical conservative surgery: A case report and review of literature
- PMID: 35979304
- PMCID: PMC9294896
- DOI: 10.12998/wjcc.v10.i19.6636
Giant retroperitoneal liposarcoma treated with radical conservative surgery: A case report and review of literature
Abstract
Background: Retroperitoneal liposarcoma (RLPS) is a rare malignant tumor of the connective tissue and usually grows to a large size, undetected. Diagnosis is currently based on collective findings from clinical examinations and computed tomography (CT) and magnetic resonance imaging, the latter of which show a fat density mass and possible surrounding organ involvement. Surgical resection is the main therapeutic strategy. The efficacy and safety of further therapeutic choices, such as chemotherapy and radiotherapy, are still controversial.
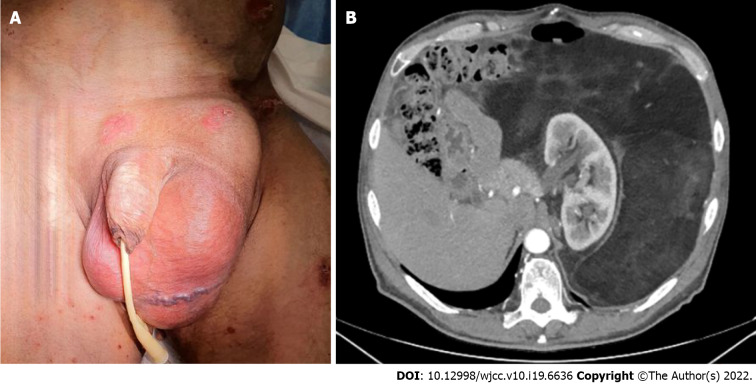
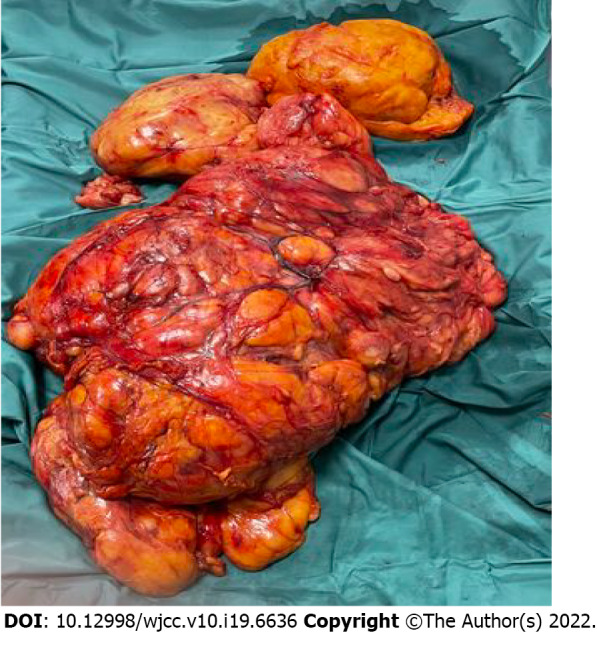
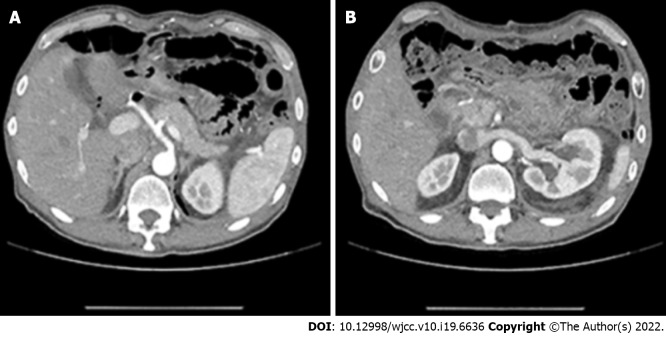
Case summary: A 61-year-old man presented with complaint of a large left inguinal mass that had appeared suddenly, after a slight exertion. Ultrasonography revealed an omental inguinal hernia. During further clinical examination, an enormous palpable abdominal mass, continuing from the left inguinal location, was observed. CT revealed a giant RLPS, with remarkable mass effect and wide visceral dislocation. After multidisciplinary consultation, surgical intervention was performed. Subsequent neoadjuvant chemotherapy and radiotherapy were precluded by the mass' large size and retroperitoneal localization, features typically associated with non-response to these types of treatment. Instead, the patient underwent conservative treatment via radical surgical excision. After 1 year, his clinical condition remained good, with no radiological signs of recurrence.
Conclusion: Conservative treatment via surgery resulted in a successful outcome for a large RLPS.
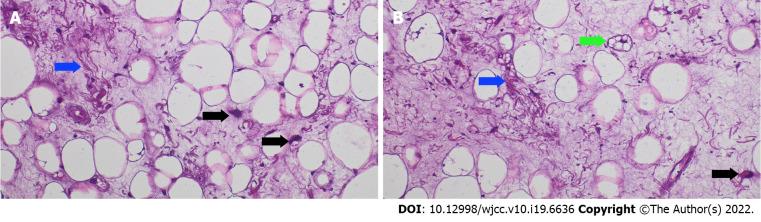
Keywords: Case report; Differentiated liposarcoma; Giant sarcoma; Retroperitoneal liposarcoma; Retroperitoneal sarcoma surgical outcome; Sarcoma diagnosis; Sarcoma surgical treatment.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
A case of enormous retroperitoneal liposarcoma with prolapse from the left inguinal canal following hernia repair.Surg Case Rep. 2024 Apr 24;10(1):101. doi: 10.1186/s40792-024-01891-0. Surg Case Rep. 2024. PMID: 38656390 Free PMC article.
-
Giant retroperitoneal well-differentiated liposarcoma presenting in emergency with intestinal occlusion: Case report and review of the literature.Int J Surg Case Rep. 2022 Jun;95:107152. doi: 10.1016/j.ijscr.2022.107152. Epub 2022 May 3. Int J Surg Case Rep. 2022. PMID: 35580411 Free PMC article.
-
Case report and literature review: Conversion surgery for initially unresectable huge retroperitoneal liposarcoma after preoperative radiotherapy.Front Oncol. 2023 Jan 6;12:1096411. doi: 10.3389/fonc.2022.1096411. eCollection 2022. Front Oncol. 2023. PMID: 36686723 Free PMC article.
-
Giant retroperitoneal sarcoma: a case report and review of the management of retroperitoneal sarcomas.Am Surg. 2002 Jan;68(1):52-6. Am Surg. 2002. PMID: 12467318 Review.
-
[Epididymal liposarcoma with metastases to the retroperitoneal space and peritoneal cavity: A case report and literature review].Zhonghua Nan Ke Xue. 2017 Dec;23(12):1103-1106. Zhonghua Nan Ke Xue. 2017. PMID: 29738182 Review. Chinese.
Cited by
-
A case of enormous retroperitoneal liposarcoma with prolapse from the left inguinal canal following hernia repair.Surg Case Rep. 2024 Apr 24;10(1):101. doi: 10.1186/s40792-024-01891-0. Surg Case Rep. 2024. PMID: 38656390 Free PMC article.
-
Dark Topics on Giant Retroperitoneal Liposarcoma: A Systematic Review of 157 Cases.Cancers (Basel). 2025 Feb 21;17(5):740. doi: 10.3390/cancers17050740. Cancers (Basel). 2025. PMID: 40075588 Free PMC article. Review.
-
Giant retroperitoneal liposarcoma with multiple organ involvement: a case report and literature review.BMC Nephrol. 2024 Aug 29;25(1):281. doi: 10.1186/s12882-024-03701-z. BMC Nephrol. 2024. PMID: 39210338 Free PMC article. Review.
-
Management challenges of a giant retroperitoneal liposarcoma: A case report and review of the literature.Int J Surg Case Rep. 2024 Dec;125:110629. doi: 10.1016/j.ijscr.2024.110629. Epub 2024 Nov 19. Int J Surg Case Rep. 2024. PMID: 39566432 Free PMC article.
References
-
- Hazen B, Cocieru A. Giant Retroperitoneal Sarcoma. J Gastrointest Surg. 2017;21:602–603. - PubMed
-
- Peterson JJ, Kransdorf MJ, Bancroft LW, O'Connor MI. Malignant fatty tumors: classification, clinical course, imaging appearance and treatment. Skeletal Radiol. 2003;32:493–503. - PubMed
-
- von Mehren M, Randall RL, Benjamin RS, Boles S, Bui MM, Ganjoo KN, George S, Gonzalez RJ, Heslin MJ, Kane JM, Keedy V, Kim E, Koon H, Mayerson J, McCarter M, McGarry SV, Meyer C, Morris ZS, O'Donnell RJ, Pappo AS, Paz IB, Petersen IA, Pfeifer JD, Riedel RF, Ruo B, Schuetze S, Tap WD, Wayne JD, Bergman MA, Scavone JL. Soft Tissue Sarcoma, Version 2.2018, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2018;16:536–563. - PubMed
-
- Fletcher CDM, Bridge JA, Hogendoorn PCW, Mertens F. Editors. WHO Classification of Soft Tissue and Bone. Switzerland: WHO, 2013.
Publication types
LinkOut - more resources
Full Text Sources
