

Successful first-line treatment of simultaneous multiple primary malignancies of lung adenocarcinoma and renal clear cell carcinoma: A case report
- PMID: 35979370
- PMCID: PMC9376962
- DOI: 10.3389/fimmu.2022.956519
Successful first-line treatment of simultaneous multiple primary malignancies of lung adenocarcinoma and renal clear cell carcinoma: A case report
Abstract
Background: Multiple Primary Malignancies (MPMs) refer to the occurrence of two or more primary malignancies in the same organ or multiple organs and tissues of the same patient simultaneously or sequentially, with an incidence rate ranging from 2-17%. According to the difference in the time of occurrence of each primary tumor, MPMs can be classified as simultaneous malignancies and heterochronic malignancies. The former refers to the occurrence of two or more malignancies one after another within 6 months, while the latter refers to the occurrence of two malignancies at an interval of more than 6 months. Currently, there is a lack of effective treatment options for MPMs both nationally and internationally.
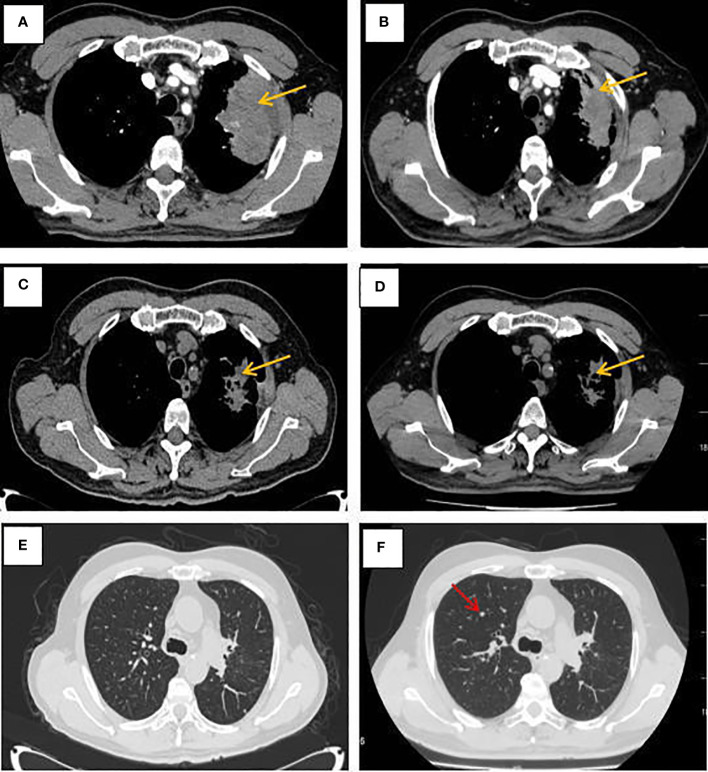
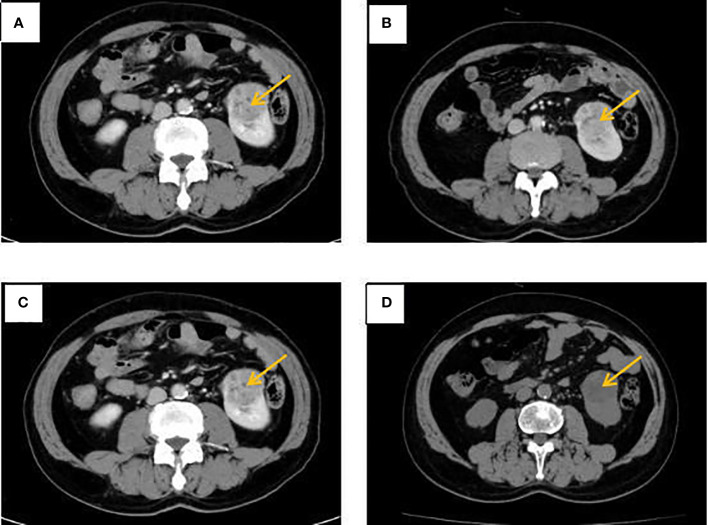
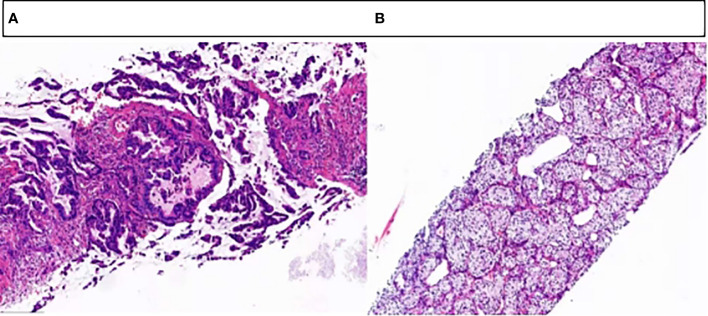
Case presentation: The patient was a 65-year-old male smoker with a definite diagnosis of advanced lung adenocarcinoma with kirsten rat sarcoma viral oncogene (KRAS) mutation, concomitant with primary renal clear cell carcinoma (RCCC), who had a progression-free survival (PFS) for 7 months after first-line treatment with albumin-bound paclitaxel and cisplatin in combination with sintilimab.
Conclusion: In this paper, we report a case of advanced lung adenocarcinoma combined with RCCC as a concurrent double primary malignancy, which achieved a satisfactory outcome after first-line chemotherapy combined with immunotherapy, with the aim of exploring effective treatment modalities for this type of MPMs, in order to improve the survival and prognosis of the patient.
Keywords: chemotherapy; immunotherapy; lung adenocarcinoma; multiple primary malignancies; renal clear cell carcinoma.
Copyright © 2022 Ye, Liu, Yin, Song, Lu, Yang and Chen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Marostica E, Barber R, Denize T, Kohane IS, Signoretti S, Golden JA, et al. . Development of a histopathology informatics pipeline for classification and prediction of clinical outcomes in subtypes of renal cell carcinoma. Clin Cancer Res (2021) 27(10):2868–78. doi: 10.1158/1078-0432.CCR-20-4119 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous