

Metabolic syndrome and cardiovascular morbidity in patients with congenital adrenal hyperplasia
- PMID: 35979433
- PMCID: PMC9376294
- DOI: 10.3389/fendo.2022.934675
Metabolic syndrome and cardiovascular morbidity in patients with congenital adrenal hyperplasia
Abstract
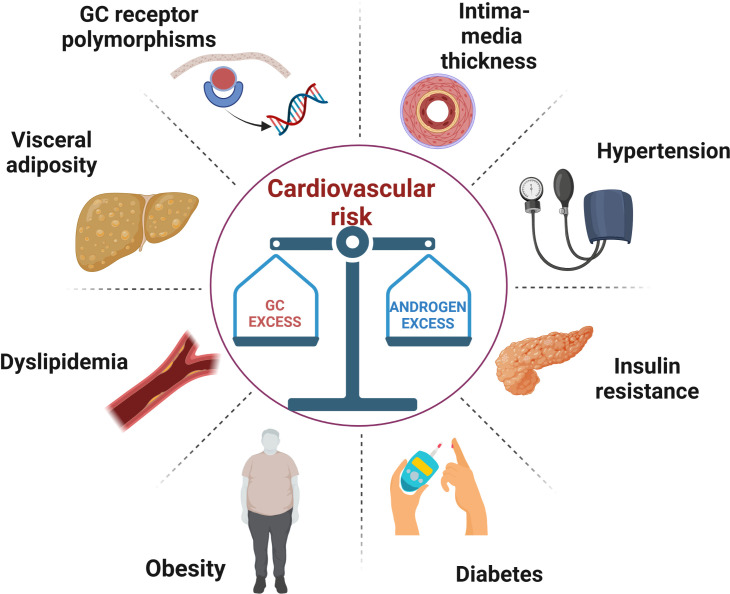
Since the introduction of glucocorticoid (GC) replacement therapy, congenital adrenal hyperplasia (CAH) is no longer a fatal disease. The development of neonatal screening programs and the amelioration of GC treatment strategies have improved significantly life expectancy in CAH patients. Thanks to these achievements, CAH patients are now in their adulthood, but an increased incidence of cardiovascular risk factors has been reported compared to general population in this stage of life. The aim of CAH treatment is to both prevent adrenal insufficiency and suppress androgen excess; in this delicate balance, under- as well as overtreatment might be equally harmful to long-term cardiovascular health. This work examines the prevalence of metabolic features and cardiovascular events, their correlation with hormone levels and GC replacement regimen in CAH patients and focuses on precocious markers to early detect patients at higher risk and new potential treatment approaches.
Keywords: cardiovascular risk; congenital adrenal hyperplasia (CAH)–21-alpha hydroxylase deficiency; diabetes mellitus; glucocorticoid therapy; metabolic syndrome; obesity.
Copyright © 2022 Barbot, Mazzeo, Lazzara, Ceccato and Scaroni.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous