

Incisional hernia following colorectal cancer surgery according to suture technique: Hughes Abdominal Repair Randomized Trial (HART)
- PMID: 35979802
- PMCID: PMC10364691
- DOI: 10.1093/bjs/znac198
Incisional hernia following colorectal cancer surgery according to suture technique: Hughes Abdominal Repair Randomized Trial (HART)
Erratum in
-
Corrigendum to: Incisional hernia following colorectal cancer surgery according to suture technique: Hughes Abdominal Repair Randomized Trial (HART).Br J Surg. 2022 Dec 13;110(1):126. doi: 10.1093/bjs/znac378. Br J Surg. 2022. PMID: 36323528 Free PMC article. No abstract available.
Abstract
Background: Incisional hernias cause morbidity and may require further surgery. HART (Hughes Abdominal Repair Trial) assessed the effect of an alternative suture method on the incidence of incisional hernia following colorectal cancer surgery.
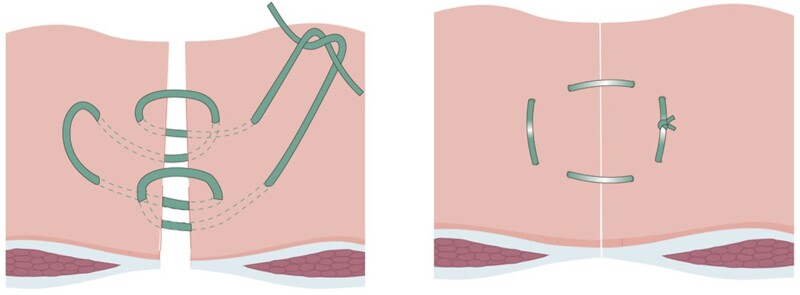
Methods: A pragmatic multicentre single-blind RCT allocated patients undergoing midline incision for colorectal cancer to either Hughes closure (double far-near-near-far sutures of 1 nylon suture at 2-cm intervals along the fascia combined with conventional mass closure) or the surgeon's standard closure. The primary outcome was the incidence of incisional hernia at 1 year assessed by clinical examination. An intention-to-treat analysis was performed.
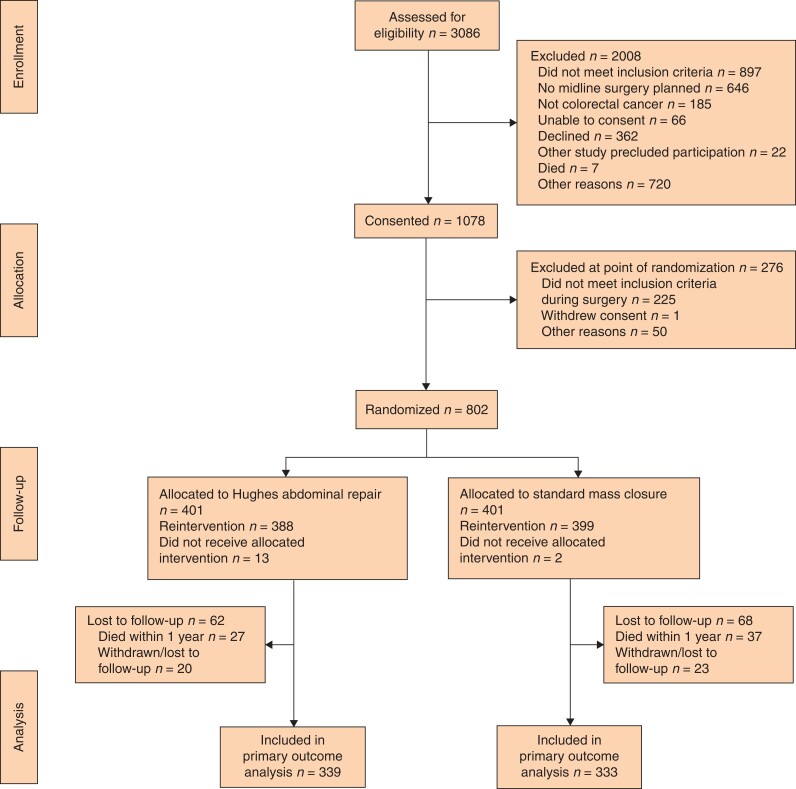
Results: Between August 2014 and February 2018, 802 patients were randomized to either Hughes closure (401) or the standard mass closure group (401). At 1 year after surgery, 672 patients (83.7 per cent) were included in the primary outcome analysis; 50 of 339 patients (14.8 per cent) in the Hughes group and 57 of 333 (17.1 per cent) in the standard closure group had incisional hernia (OR 0.84, 95 per cent c.i. 0.55 to 1.27; P = 0.402). At 2 years, 78 patients (28.7 per cent) in the Hughes repair group and 84 (31.8 per cent) in the standard closure group had incisional hernia (OR 0.86, 0.59 to 1.25; P = 0.429). Adverse events were similar in the two groups, apart from the rate of surgical-site infection, which was higher in the Hughes group (13.2 versus 7.7 per cent; OR 1.82, 1.14 to 2.91; P = 0.011).
Conclusion: The incidence of incisional hernia after colorectal cancer surgery is high. There was no statistical difference in incidence between Hughes closure and mass closure at 1 or 2 years.
Registration number: ISRCTN25616490 (http://www.controlled-trials.com).
Plain language summary
After bowel cancer surgery, bulges known as hernias can occur at the site of the scar. Many patients find this uncomfortable and embarrassing. These hernias can also need further operations, sometimes as an emergency. This trial aimed to find out whether one way of closing the scars was better than another at stopping hernias developing. A total of 802 patients from 28 different hospitals in the UK joined the trial. The patients all had bowel cancer, and at the end of the operation had either a method known as the Hughes closure to close the incision or the method that the surgeon normally used. There was no difference between the two types of closure. The trial has shown that the chance of getting a hernia after a bowel cancer operation is still much higher than surgeons or patients would like.
© The Author(s) 2022. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures
Comment in
-
Comment on: Incisional hernia following colorectal cancer surgery according to suture technique: Hughes Abdominal Repair Randomized Trial (HART).Br J Surg. 2023 Feb 15;110(3):386. doi: 10.1093/bjs/znac441. Br J Surg. 2023. PMID: 36519222 No abstract available.
References
-
- Korenkov M, Paul A, Sauerland S, Neugebauer E, Arndt M, Chevrel JP et al. Classification and surgical treatment of incisional hernia. Results of an experts’ meeting. Langenbecks Arch Surg 2001;386:65–73 - PubMed
-
- Geçim I E, Koçak S, Ersoz S, Bumin C, Aribal D. Recurrence after incisional hernia repair: results and risk factors. Surg Today 1996;26:607–609 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
