

The Use of a Self-triage Tool to Predict COVID-19 Cases and Hospitalizations in the State of Georgia
- PMID: 35980417
- PMCID: PMC9391013
- DOI: 10.5811/westjem.2022.4.55001
The Use of a Self-triage Tool to Predict COVID-19 Cases and Hospitalizations in the State of Georgia
Abstract
Introduction: The coronavirus 2019 (COVID-19) pandemic has created significant burden on healthcare systems throughout the world. Syndromic surveillance, which collects real-time data based on a range of symptoms rather than laboratory diagnoses, can help provide timely information in emergency response. We examined the effectiveness of a web-based COVID-19 symptom checking tool (C19Check) in the state of Georgia (GA) in predicting COVID-19 cases and hospitalizations.
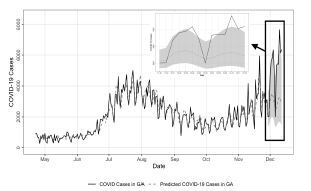
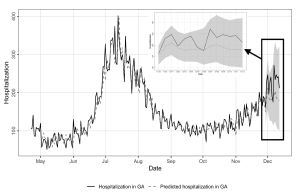
Methods: We analyzed C19Check use data, COVID-19 cases, and hospitalizations from April 22-November 28, 2020. Cases and hospitalizations in GA were extracted from the Georgia Department of Public Health data repository. We used the Granger causality test to assess whether including C19Check data can improve predictions compared to using previous COVID-19 cases and hospitalizations data alone. Vector autoregression (VAR) models were fitted to forecast cases and hospitalizations from November 29 - December 12, 2020. We calculated mean absolute percentage error to estimate the errors in forecast of cases and hospitalizations.
Results: There were 25,861 C19Check uses in GA from April 22-November 28, 2020. Time-lags tested in Granger causality test for cases (6-8 days) and hospitalizations (10-12 days) were significant (P= <0.05); the mean absolute percentage error of fitted VAR models were 39.63% and 15.86%, respectively.
Conclusion: The C19Check tool was able to help predict COVID-19 cases and related hospitalizations in GA. In settings where laboratory tests are limited, a real-time, symptom-based assessment tool can provide timely and inexpensive data for syndromic surveillance to guide pandemic response. Findings from this study demonstrate that online symptom-checking tools can be a source of data for syndromic surveillance, and the data may help improve predictions of cases and hospitalizations.
Conflict of interest statement
Figures
Similar articles
-
A Self-Assessment Web-Based App to Assess Trends of the COVID-19 Pandemic in France: Observational Study.J Med Internet Res. 2021 Mar 12;23(3):e26182. doi: 10.2196/26182. J Med Internet Res. 2021. PMID: 33709945 Free PMC article.
-
Implementation of a Self-Triage Web Application for Suspected COVID-19 and Its Impact on Emergency Call Centers: Observational Study.J Med Internet Res. 2020 Nov 23;22(11):e22924. doi: 10.2196/22924. J Med Internet Res. 2020. PMID: 33147165 Free PMC article.
-
Secondary Use of COVID-19 Symptom Incidence Among Hospital Employees as an Example of Syndromic Surveillance of Hospital Admissions Within 7 Days.JAMA Netw Open. 2021 Jun 1;4(6):e2113782. doi: 10.1001/jamanetworkopen.2021.13782. JAMA Netw Open. 2021. PMID: 34137827 Free PMC article.
-
Vector Autoregression for Forecasting the Number of COVID-19 Cases and Analyzing Behavioral Indicators in the Philippines: Ecologic Time-Trend Study.JMIR Form Res. 2023 Jun 27;7:e46357. doi: 10.2196/46357. JMIR Form Res. 2023. PMID: 37368473 Free PMC article.
-
Hospitalizations from covid-19: a health planning tool.Rev Saude Publica. 2022 Jun 13;56:51. doi: 10.11606/s1518-8787.2022056004315. eCollection 2022. Rev Saude Publica. 2022. PMID: 35703605 Free PMC article. Review.
Cited by
-
AI-driven healthcare: Fairness in AI healthcare: A survey.PLOS Digit Health. 2025 May 20;4(5):e0000864. doi: 10.1371/journal.pdig.0000864. eCollection 2025 May. PLOS Digit Health. 2025. PMID: 40392801 Free PMC article. Review.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous