

Incidence of Neonatal Developmental Dysplasia of the Hip and Late Detection Rates Based on Screening Strategy: A Systematic Review and Meta-analysis
- PMID: 35980635
- PMCID: PMC9389349
- DOI: 10.1001/jamanetworkopen.2022.27638
Incidence of Neonatal Developmental Dysplasia of the Hip and Late Detection Rates Based on Screening Strategy: A Systematic Review and Meta-analysis
Abstract
Importance: Universal ultrasonographic screening for developmental dysplasia of the hip (DDH) has gained increasing popularity despite the lack of benefit in terms of reducing the rates of late-detected cases (age ≥12 weeks) in randomized clinical trials.
Objective: To report the reported incidence of DDH in the English scientific literature and compare rates of late-detected cases in settings with different DDH screening strategies.
Data sources: PubMed, Scopus, and Web of Science databases were searched on November 25 and 27, 2021. No time filters were used in the search.
Study selection: All observational studies reporting the incidence of early-detected or late-detected (age ≥12 weeks) DDH were included. Non-English reports were excluded if the abstract did not include enough information to be included for analysis.
Data extraction and synthesis: The number of newborns screened and the detection rates were extracted. Meta-analysis calculated the pooled incidence of DDH per 1000 newborns with 95% CIs using a random- or fixed-effects model. This study is reported according to the PRISMA and MOOSE guidelines.
Main outcomes and measures: The main outcome measures were early detection, early treatment, late detection, and operative treatment incidences.
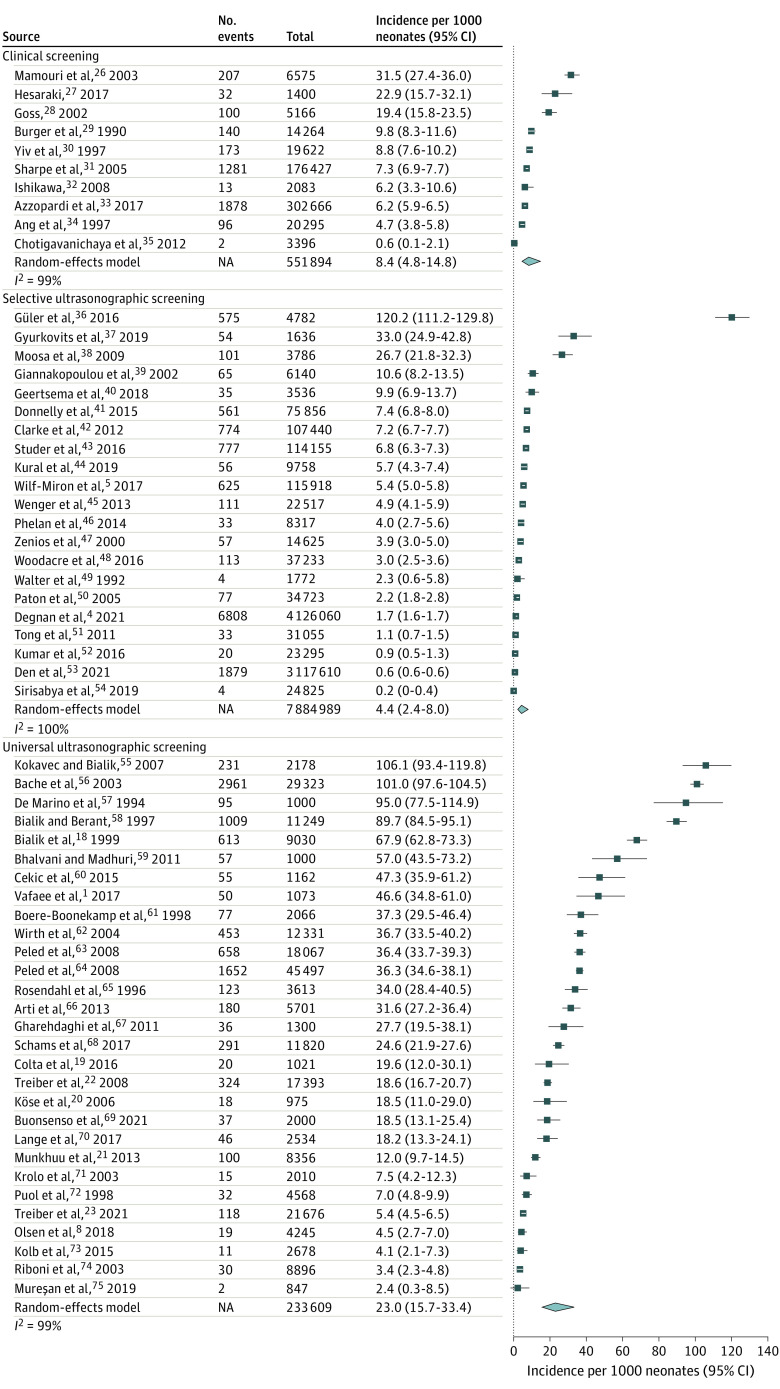
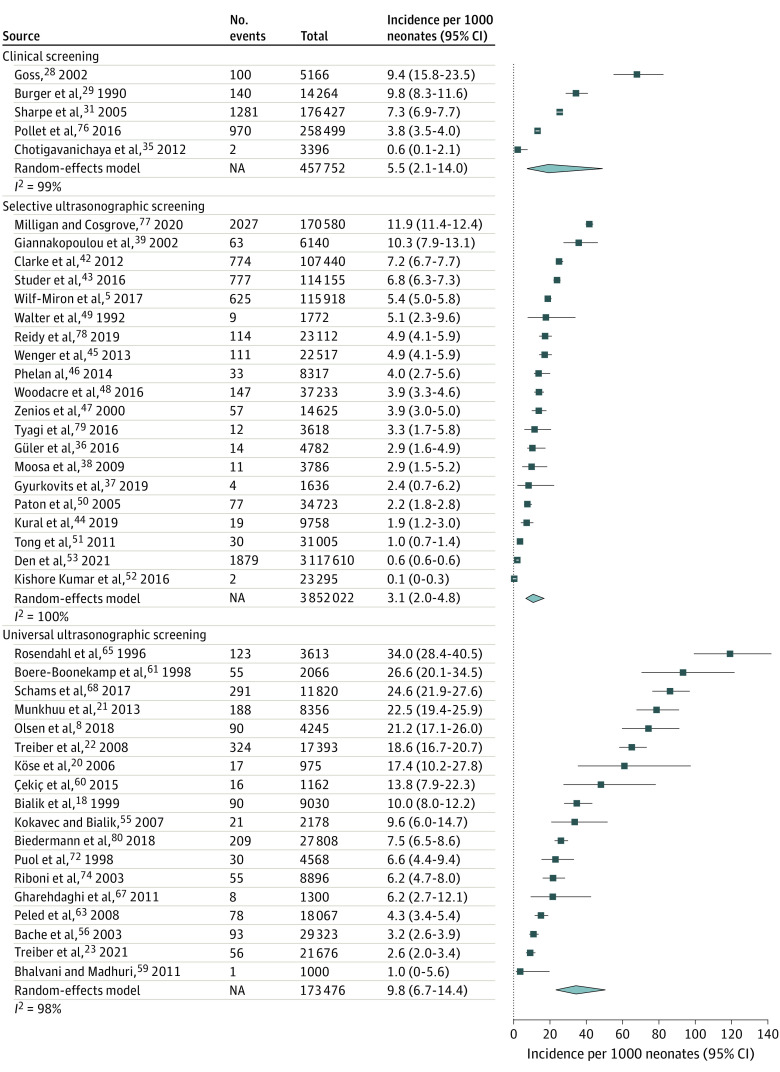
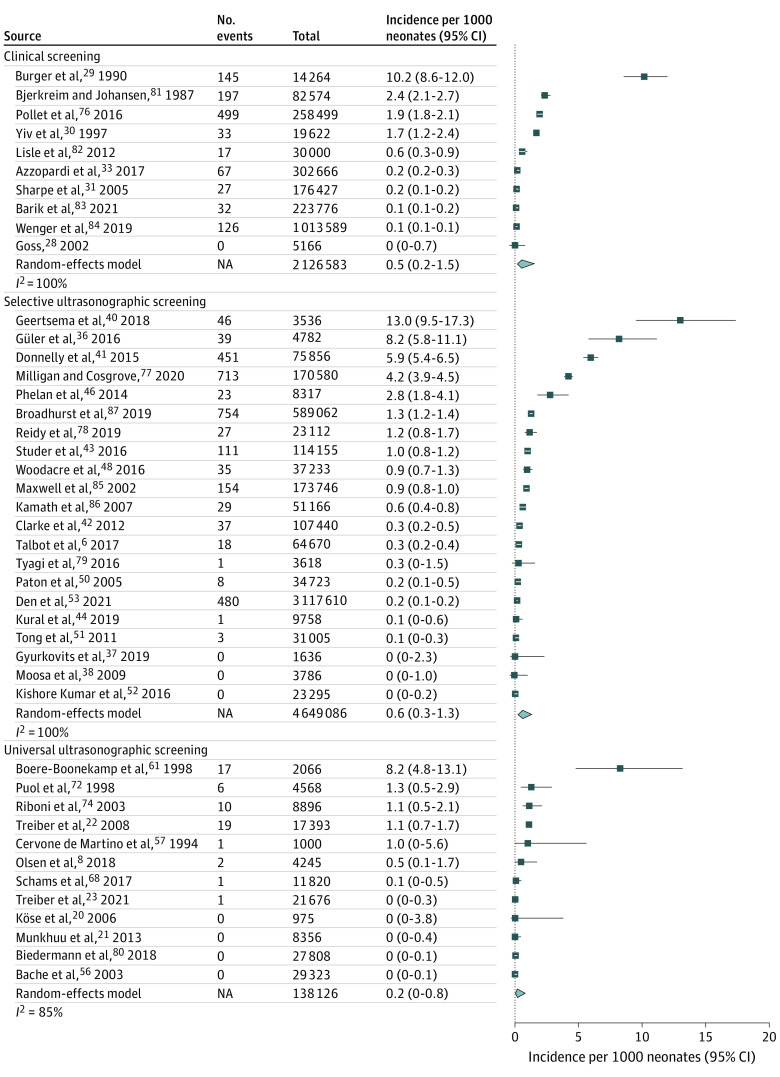
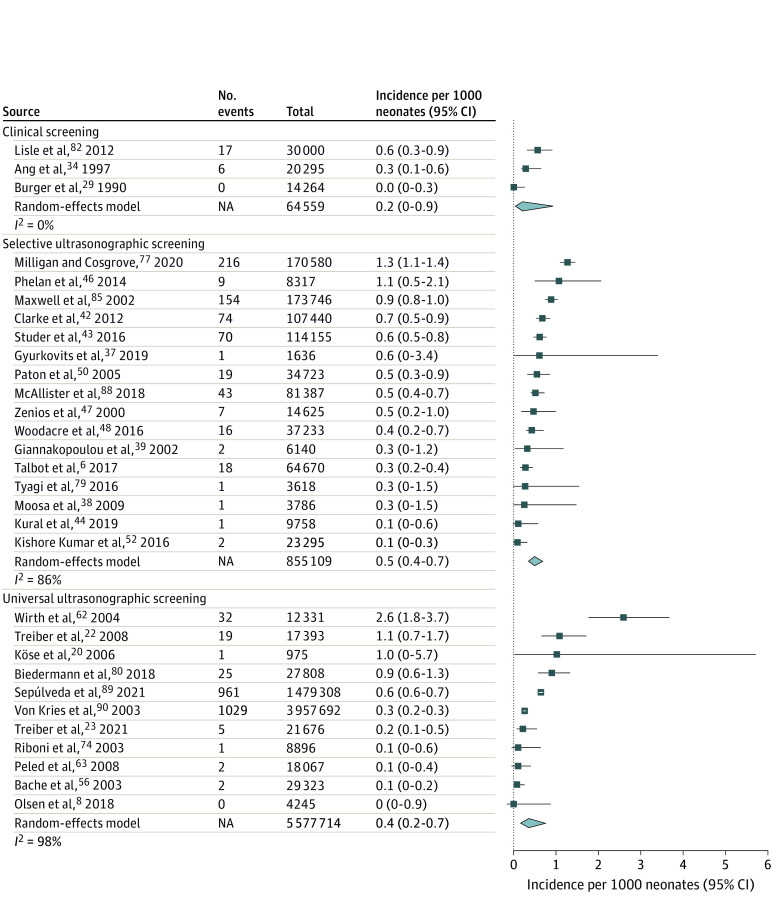
Results: A total of 1899 studies were identified, 203 full texts were assessed, and 76 studies with 16 901 079 infants were included in final analyses. The early detection rate was 8.4 (95% CI, 4.8-14.8) infants with DDH per 1000 newborns with clinical screening, 4.4 (95% CI, 2.4-8.0) infants with DDH per 1000 newborns with selective ultrasonographic screening, and 23.0 (95% CI, 15.7-33.4) infants with DDH per 1000 newborns with universal ultrasonographic screening. Rates for nonoperative treatment were 5.5 (95% CI, 2.1-14) treatments per 1000 newborns with clinical screening, 3.1 (95% CI, 2.0-4.8) treatments per 1000 newborns with selective ultrasonographic screening, and 9.8 (95% CI, 6.7-14.4) treatments per 1000 newborns with universal ultrasonographic screening. The incidence of late-detected DDH was 0.5 (95% CI, 0.2-1.5) infants with DDH per 1000 newborns with clinical screening, 0.6 (95% CI, 0.3-1.3) infants with DDH per 1000 newborns with selective ultrasonographic screening, and 0.2 (95% CI, 0.0-0.8) infants with DDH per 1000 newborns with universal ultrasonographic screening. The corresponding incidences of operative treatment were 0.2 (95% CI, 0.0-0.9) operations per 1000 newborns with clinical screening, 0.5 (95% CI, 0.4-0.7) operations per 1000 newborns with selective ultrasonographic screening, and 0.4 (95% CI, 0.2-0.7) operations per 1000 newborns with universal ultrasonographic screening.
Conclusions and relevance: This meta-analysis found that early detection rates and nonoperative treatments were higher with universal screening. The late detection and operative treatment rates with universal screening were similar to those among selectively and clinically screened newborns. Based on these results, universal screening may cause initial overtreatment without reducing the rates of late detection and operative treatment.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
