

Association of Insurance Coverage With Adoption of Sleeve Gastrectomy vs Gastric Bypass for Patients Undergoing Bariatric Surgery
- PMID: 35980640
- PMCID: PMC9389353
- DOI: 10.1001/jamanetworkopen.2022.25964
Association of Insurance Coverage With Adoption of Sleeve Gastrectomy vs Gastric Bypass for Patients Undergoing Bariatric Surgery
Abstract
Importance: Instrumental variables can control for selection bias in observational research. However, valid instruments are challenging to identify.
Objective: To evaluate regional variation in sleeve gastrectomy following insurance coverage implementation as an instrumental variable in comparative effectiveness research.
Design, setting, and participants: This serial cross-sectional study included adult patients in a national Medicare claims database who underwent sleeve gastrectomy or Roux-en-Y gastric bypass from 2012 to 2017. Data analysis was performed from January to June 2021.
Exposures: Laparoscopic sleeve gastrectomy and Roux-en-Y gastric bypass.
Main outcomes and measures: The association of the instrumental variable with treatment (ie, undergoing sleeve gastrectomy), as well as mortality, complications, emergency department visits, hospitalization, reinterventions, and surgical revision.
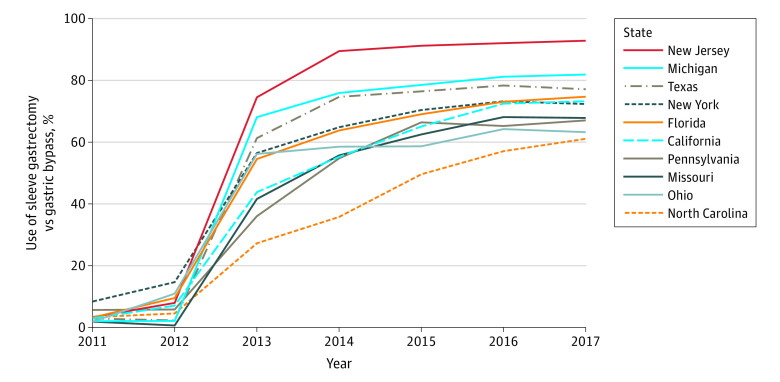
Results: A total of 76 077 patients underwent bariatric surgery, of whom 44 367 underwent sleeve gastrectomy (mean [SD] age, 56.9 [11.9] years; 32 559 [73.5%] women) and 31 710 underwent gastric bypass (mean (SD) age, 55.9 (11.8) years; 23 750 [74.9%] women). After insurance coverage initiation, there was substantial regional and temporal variation in adoption of sleeve gastrectomy. Prior-year state-level utilization of sleeve gastrectomy was highly associated with undergoing sleeve gastrectomy (Kleibergen-Paap Wald F statistic, 910.3). All but 2 patient characteristics (race and diagnosis of depression) were well-balanced between the top and bottom quartiles of the instrumental variable. Regarding 1-year outcomes, compared with patients undergoing gastric bypass, patients undergoing sleeve gastrectomy had a lower 1-year risk of mortality (0.9%; 95% CI, 0.8%-1.1% vs 1.7%; 95% CI, 1.3%-2.0%), complications (11.6%; 95% CI, 10.9%-12.3% vs 14.1%; 95% CI, 13.0%-15.3%), emergency department visits (48.3%; 95% CI, 46.9%-49.8% vs 53.6%; 95% CI, 52.3%-55.0%), hospitalization (23.4%; 95% CI, 22.4%-24.4% vs 26.5%; 95% CI, 25.1%-28.0%), and reinterventions (8.7%; 95% CI, 8.0%-9.4% vs 12.2%; 95% CI, 11.2%-13.3%). The risk of revision was not different between groups (0.6%; 95% CI, 0.3%-0.8% vs 0.4%; 95% CI, 0.3%-0.6%).
Conclusions and relevance: In this cross-sectional study of patients undergoing bariatric surgery, there was significant geographic variation in the use of sleeve gastrectomy following initiation of insurance coverage, which served as a strong instrument to compare 2 bariatric surgical procedures. This approach could be applied to other areas of health services research to serve as a complement to clinical trials.
Conflict of interest statement
Figures
Comment in
-
Potential Bias of Instrumental Variable Analysis in Comparative Effectiveness Research for Bariatric Surgery.JAMA Netw Open. 2022 Aug 1;5(8):e2225970. doi: 10.1001/jamanetworkopen.2022.25970. JAMA Netw Open. 2022. PMID: 35980642 No abstract available.
Similar articles
-
Comparative Safety of Sleeve Gastrectomy and Gastric Bypass Up to 5 Years After Surgery in Patients With Severe Obesity.JAMA Surg. 2021 Dec 1;156(12):1160-1169. doi: 10.1001/jamasurg.2021.4981. JAMA Surg. 2021. PMID: 34613354 Free PMC article.
-
Comparative effectiveness of sleeve gastrectomy vs Roux-en-Y gastric bypass in patients giving birth after bariatric surgery: reinterventions and obstetric outcomes.Surg Endosc. 2022 Sep;36(9):6954-6968. doi: 10.1007/s00464-022-09063-7. Epub 2022 Jan 31. Surg Endosc. 2022. PMID: 35099628
-
Bariatric Surgery in Medicare Patients: Examining Safety and Healthcare Utilization in the Disabled and Elderly.Ann Surg. 2022 Jul 1;276(1):133-139. doi: 10.1097/SLA.0000000000004526. Epub 2020 Nov 17. Ann Surg. 2022. PMID: 33214440 Free PMC article.
-
Comparative analysis of weight loss and resolution of comorbidities between laparoscopic sleeve gastrectomy and Roux-en-Y gastric bypass: A systematic review and meta-analysis based on 18 studies.Int J Surg. 2020 Apr;76:101-110. doi: 10.1016/j.ijsu.2020.02.035. Epub 2020 Mar 6. Int J Surg. 2020. PMID: 32151750
-
Short-Term Outcomes of Conversion of Failed Gastric Banding to Laparoscopic Sleeve Gastrectomy or Roux-En-Y Gastric Bypass: a Meta-Analysis.Obes Surg. 2019 Feb;29(2):420-425. doi: 10.1007/s11695-018-3538-8. Obes Surg. 2019. PMID: 30293135
Cited by
-
Policy Interventions to Enhance Medical Care for People With Obesity in the United States-Challenges, Opportunities, and Future Directions.Milbank Q. 2024 Jun;102(2):336-350. doi: 10.1111/1468-0009.12693. Epub 2024 Feb 8. Milbank Q. 2024. PMID: 38332667 Free PMC article.
-
Sleeve Gastrectomy Protects Against Hypertension in Rats due to Changes in the Gut Microbiome.J Surg Res. 2024 Sep;301:118-126. doi: 10.1016/j.jss.2024.05.044. Epub 2024 Jun 25. J Surg Res. 2024. PMID: 38925098 Free PMC article.
-
Obstacles Faced by Young Bariatric Surgeons in Greece: A Call for Change.Obes Surg. 2025 May;35(5):1989-1992. doi: 10.1007/s11695-025-07820-w. Epub 2025 Mar 27. Obes Surg. 2025. PMID: 40146456 No abstract available.
-
Association Between Racial and Socioeconomic Disparities and Hospital Performance in Treatment and Outcomes for Patients with Colon Cancer.Ann Surg Oncol. 2024 Feb;31(2):1075-1086. doi: 10.1245/s10434-023-14607-9. Epub 2023 Dec 7. Ann Surg Oncol. 2024. PMID: 38062293
-
Feasibility of same-day discharge after laparoscopic sleeve gastrectomy in the Netherlands.Surg Endosc. 2024 Feb;38(2):872-879. doi: 10.1007/s00464-023-10590-0. Epub 2023 Dec 11. Surg Endosc. 2024. PMID: 38082016
References
-
- Staiger D, Stock JH. Instrumental Variables Regression With Weak Instruments. National Bureau of Economic Research; 1994.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
