

MCP-1/CCR2 axis inhibition sensitizes the brain microenvironment against melanoma brain metastasis progression
- PMID: 35980743
- PMCID: PMC9536270
- DOI: 10.1172/jci.insight.154804
MCP-1/CCR2 axis inhibition sensitizes the brain microenvironment against melanoma brain metastasis progression
Abstract
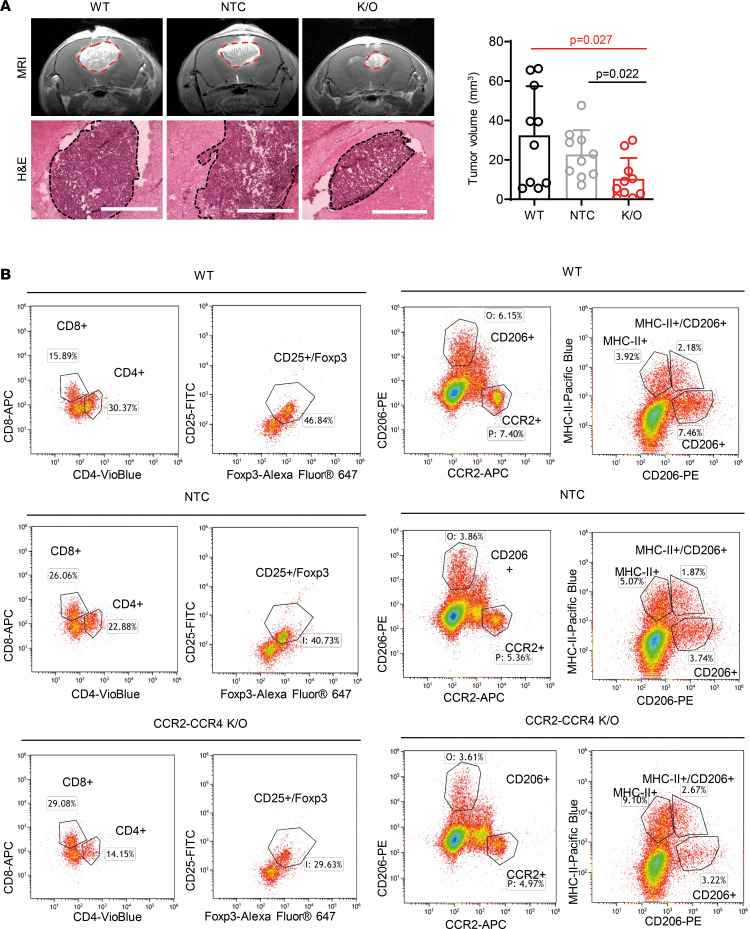
Development of resistance to chemo- and immunotherapies often occurs following treatment of melanoma brain metastasis (MBM). The brain microenvironment (BME), particularly astrocytes, cooperate toward MBM progression by upregulating secreted factors, among which we found that monocyte chemoattractant protein-1 (MCP-1) and its receptors, CCR2 and CCR4, were overexpressed in MBM compared with primary lesions. Among other sources of MCP-1 in the brain, we show that melanoma cells altered astrocyte secretome and evoked MCP-1 expression and secretion, which in turn induced CCR2 expression in melanoma cells, enhancing in vitro tumorigenic properties, such as proliferation, migration, and invasion of melanoma cells. In vivo pharmacological blockade of MCP-1 or molecular knockout of CCR2/CCR4 increased the infiltration of cytotoxic CD8+ T cells and attenuated the immunosuppressive phenotype of the BME as shown by decreased infiltration of Tregs and tumor-associated macrophages/microglia in several models of intracranially injected MBM. These in vivo strategies led to decreased MBM outgrowth and prolonged the overall survival of the mice. Our findings highlight the therapeutic potential of inhibiting interactions between BME and melanoma cells for the treatment of this disease.
Keywords: Cancer immunotherapy; Oncology; Skin cancer; Therapeutics.
Conflict of interest statement
Figures







Similar articles
-
Targeting of tumour-infiltrating macrophages via CCL2/CCR2 signalling as a therapeutic strategy against hepatocellular carcinoma.Gut. 2017 Jan;66(1):157-167. doi: 10.1136/gutjnl-2015-310514. Epub 2015 Oct 9. Gut. 2017. PMID: 26452628
-
Role of MCP-1 and CCR2 in ethanol-induced neuroinflammation and neurodegeneration in the developing brain.J Neuroinflammation. 2018 Jul 5;15(1):197. doi: 10.1186/s12974-018-1241-2. J Neuroinflammation. 2018. PMID: 29976212 Free PMC article.
-
Analysis of monocyte infiltration in MPTP mice reveals that microglial CX3CR1 protects against neurotoxic over-induction of monocyte-attracting CCL2 by astrocytes.J Neuroinflammation. 2017 Mar 21;14(1):60. doi: 10.1186/s12974-017-0830-9. J Neuroinflammation. 2017. PMID: 28320442 Free PMC article.
-
Targeting the CCL2/CCR2 Axis in Cancer Immunotherapy: One Stone, Three Birds?Front Immunol. 2021 Nov 3;12:771210. doi: 10.3389/fimmu.2021.771210. eCollection 2021. Front Immunol. 2021. PMID: 34804061 Free PMC article. Review.
-
The regulation and importance of monocyte chemoattractant protein-1.Curr Opin Hematol. 2018 Jan;25(1):44-51. doi: 10.1097/MOH.0000000000000389. Curr Opin Hematol. 2018. PMID: 28914666 Review.
Cited by
-
Vagal blockade of the brain-liver axis deters cancer-associated cachexia.Cell. 2025 Jul 29:S0092-8674(25)00805-0. doi: 10.1016/j.cell.2025.07.016. Online ahead of print. Cell. 2025. PMID: 40780194
-
Harnessing immunotherapy for brain metastases: insights into tumor-brain microenvironment interactions and emerging treatment modalities.J Hematol Oncol. 2023 Dec 16;16(1):121. doi: 10.1186/s13045-023-01518-1. J Hematol Oncol. 2023. PMID: 38104104 Free PMC article. Review.
-
Integration analysis of single-cell transcriptome reveals specific monocyte subsets associated with melanoma brain and leptomeningeal metastasis.Skin Res Technol. 2024 Apr;30(4):e13710. doi: 10.1111/srt.13710. Skin Res Technol. 2024. PMID: 38616506 Free PMC article.
-
Correlation of Immunomodulatory Cytokines with Tumor Volume and Cerebrospinal Fluid in Vestibular Schwannoma Patients.Cancers (Basel). 2024 Aug 29;16(17):3002. doi: 10.3390/cancers16173002. Cancers (Basel). 2024. PMID: 39272860 Free PMC article.
-
Tumor cell-intrinsic MELK enhanced CCL2-dependent immunosuppression to exacerbate hepatocarcinogenesis and confer resistance of HCC to radiotherapy.Mol Cancer. 2024 Jul 5;23(1):137. doi: 10.1186/s12943-024-02049-0. Mol Cancer. 2024. PMID: 38970074 Free PMC article.
References
-
- Durão C, et al. Sudden death associated with melanoma brain metastases. J Pathol Nepal. 2018;8(2):1412–1415. doi: 10.3126/jpn.v8i2.20896. - DOI
-
- Friedlander P. Advances in the Systemic Treatment of Melanoma Brain Metastases. In: Morgan LR, Sarica FB, eds. Brain and Spinal Tumors Primary and Secondary. IntechOpen; 2020.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
