

Laparoscopic entry techniques: Which should you prefer?
- PMID: 35980870
- PMCID: PMC10087714
- DOI: 10.1002/ijgo.14412
Laparoscopic entry techniques: Which should you prefer?
Abstract
Background: Despite a debate spanning two decades, no consensus has been achieved about the safest laparoscopic entry technique.
Objectives: To update the evidence about the safety of the main different laparoscopic entry techniques.
Search strategy: Six electronic databases were searched from inception to February 2021.
Selection criteria: All randomized controlled trials (RCTs) comparing different laparoscopic entry techniques were included.
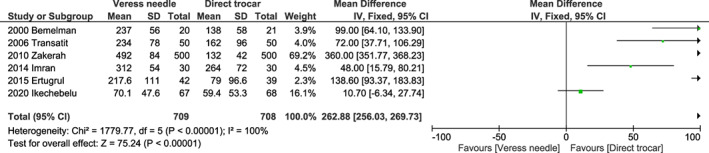
Data collection and analysis: Entry-related complications and total time for entry were compared among the different methods of entry calculating pooled odds ratios (ORs) and mean differences, with 95% confidence intervals (CIs); P < 0.05 was considered significant.
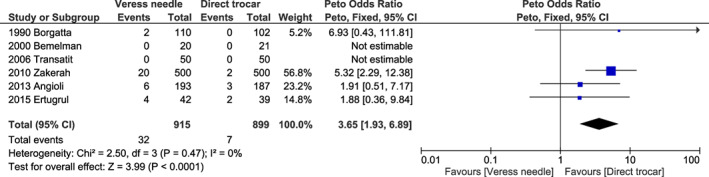
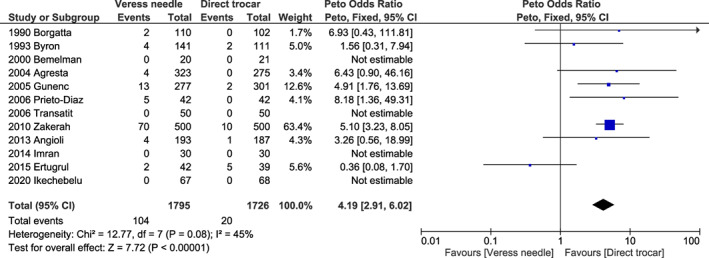
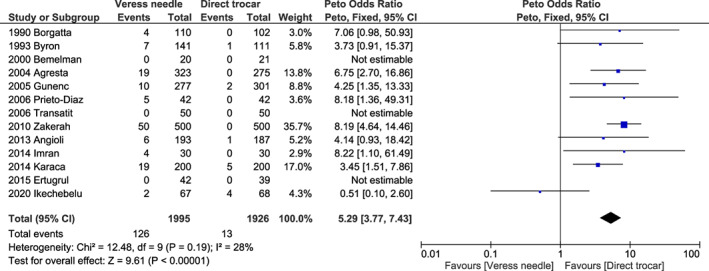
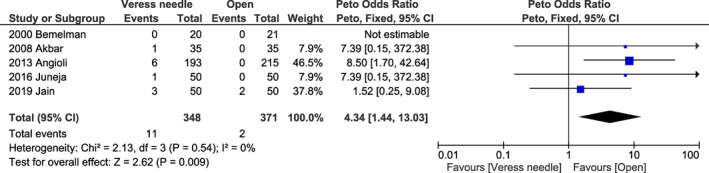
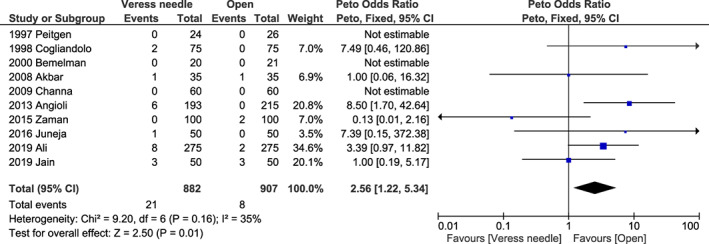
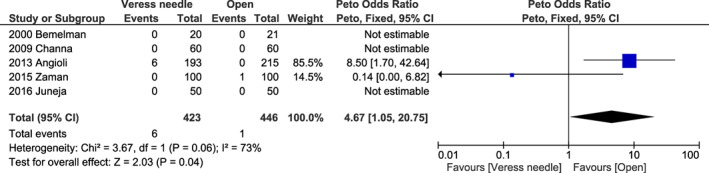
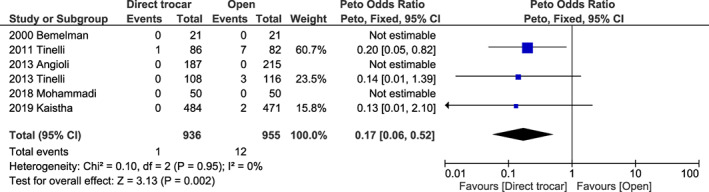
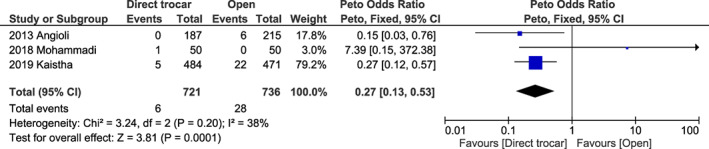
Main results: In total, 25 RCTs (6950 patients) were included. Complications considered were vascular, visceral and omental injury, failed entry, extraperitoneal insufflation, bleeding and infection at the trocar site bleeding, and incisional hernia. Compared to direct trocar, the OR for Veress needle was significantly higher for omental injury (OR 3.65, P < 0.001), for failed entry (OR 4.19, P < 0.001), and for extraperitoneal insufflation (OR 5.29, P < 0.001). Compared to the open method, the OR for Veress needle was significantly higher for omental injury (OR 4.93, P = 0.001), for failed entry (OR 2.99, P < 0.001), for extraperitoneal insufflation (OR 4.77; P = 0.04), and for incisional hernia. Compared to the open method, the OR for direct trocar was significantly lower for visceral injury (OR 0.17, P = 0.002) and for trocar site infection (OR 0.27, P = 0.001).
Conclusions: The direct trocar method may be preferred over Veress needle and open methods as a laparoscopic entry technique since it appears associated to a lower risk of complications.
Keywords: access; complications; guidelines; laparoscopy; minimally invasive; recommendation; safety; surgery.
© 2022 The Authors. International Journal of Gynecology & Obstetrics published by John Wiley & Sons Ltd on behalf of International Federation of Gynecology and Obstetrics.
Conflict of interest statement
The authors have no conflicts of interest.
Figures

Similar articles
-
Laparoscopic entry techniques.Cochrane Database Syst Rev. 2019 Jan 18;1(1):CD006583. doi: 10.1002/14651858.CD006583.pub5. Cochrane Database Syst Rev. 2019. PMID: 30657163 Free PMC article.
-
Laparoscopic entry: a review of techniques, technologies, and complications.J Obstet Gynaecol Can. 2007 May;29(5):433-447. doi: 10.1016/S1701-2163(16)35496-2. J Obstet Gynaecol Can. 2007. PMID: 17493376 Review. English, French.
-
Direct trocar insertion without previous pneumoperitoneum versus insertion after insufflation with Veress needle in laparoscopic gynecological surgery: a prospective cohort study.J Obstet Gynaecol. 2019 Oct;39(7):1000-1005. doi: 10.1080/01443615.2019.1590804. Epub 2019 Jun 18. J Obstet Gynaecol. 2019. PMID: 31210067
-
A comparison of three different entry techniques in gynecological laparoscopic surgery: a randomized prospective trial.Eur J Obstet Gynecol Reprod Biol. 2013 Dec;171(2):339-42. doi: 10.1016/j.ejogrb.2013.09.012. Epub 2013 Sep 23. Eur J Obstet Gynecol Reprod Biol. 2013. PMID: 24103531 Clinical Trial.
-
Comparison Of Operative Complications Of Direct Trocar Access Versus Veress Needle Insertion Technique For Initial Peritoneal Entry In Patients Undergoing Gynecological Laparoscopic Surgery.J Ayub Med Coll Abbottabad. 2021 Apr-Jun;33(2):311-314. J Ayub Med Coll Abbottabad. 2021. PMID: 34137551 Clinical Trial.
Cited by
-
Abdominal access in laparoscopic surgery of obese patients: a novel abdominal access technique.Ann Saudi Med. 2023 Jul-Aug;43(4):236-242. doi: 10.5144/0256-4947.2023.236. Epub 2023 Aug 3. Ann Saudi Med. 2023. PMID: 37554021 Free PMC article.
-
Comparative outcomes of Palmer, Umbilical Veress needle, and open entry techniques in robotic-assisted surgery: a propensity-matched analysis of 9482 patients.J Robot Surg. 2025 Jan 8;19(1):48. doi: 10.1007/s11701-024-02208-x. J Robot Surg. 2025. PMID: 39775229
-
Prevention and Treatment of Intraoperative Complications During Gynecological Laparoscopic Surgery: Practical Tips and Tricks-A Narrative Review.Adv Ther. 2025 May;42(5):2089-2117. doi: 10.1007/s12325-025-03165-z. Epub 2025 Mar 19. Adv Ther. 2025. PMID: 40106176 Free PMC article. Review.
References
-
- Ghezzi F, Cromi A, Siesto G, et al. Use of laparoscopy in older women undergoing gynecologic procedures: is it time to overcome initial concerns? Menopause. 2010;17:96‐103. - PubMed
-
- Canis M, Botchorishvili R, Ang C, et al. When is laparotomy needed in hysterectomy for benign uterine disease? J Minim Invasive Gynecol. 2008;15:38‐43. - PubMed
-
- Jansen FW, Kapiteyn K, Trimpos T, et al. Complication of laparoscopy: a prospective multicentre observational study. Br J Obstet Gynaecol. 1997;104:595‐600. - PubMed
-
- Palmer R. Safety in laparoscopy. J Reprod Med. 1974;13:1‐5. - PubMed
-
- Jansen FW, Kolman W, Bakkum EA, et al. Complications of laparoscopy: an inquiry about closed versus open entry technique. Am J Obstet Gynecol. 2004;190:634‐638. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
