

Approach to Hypophosphatemic Rickets
- PMID: 35981346
- PMCID: PMC9759174
- DOI: 10.1210/clinem/dgac488
Approach to Hypophosphatemic Rickets
Abstract
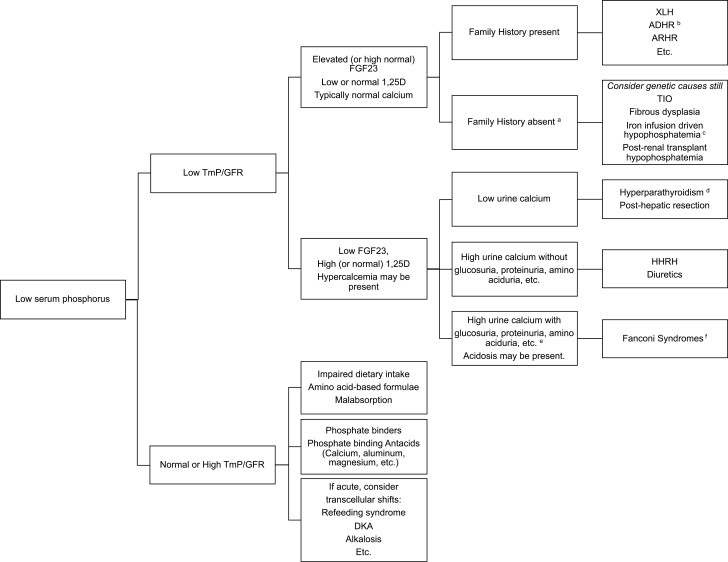
Hypophosphatemic rickets typically presents in infancy or early childhood with skeletal deformities and growth plate abnormalities. The most common causes are genetic (such as X-linked hypophosphatemia), and these typically will result in lifelong hypophosphatemia and osteomalacia. Knowledge of phosphate metabolism, including the effects of fibroblast growth factor 23 (FGF23) (an osteocyte produced hormone that downregulates renal phosphate reabsorption and 1,25-dihydroxyvitamin-D (1,25(OH)2D) production), is critical to determining the underlying genetic or acquired causes of hypophosphatemia and to facilitate appropriate treatment. Serum phosphorus should be measured in any child or adult with musculoskeletal complaints suggesting rickets or osteomalacia. Clinical evaluation incudes thorough history, physical examination, laboratory investigations, genetic analysis (especially in the absence of a guiding family history), and imaging to establish etiology and to monitor severity and treatment course. The treatment depends on the underlying cause, but often includes active forms of vitamin D combined with phosphate salts, or anti-FGF23 antibody treatment (burosumab) for X-linked hypophosphatemia. The purpose of this article is to explore the approach to evaluating hypophosphatemic rickets and its treatment options.
Keywords: X-linked hypophosphatemia; burosumab; fibroblast growth factor 23; hypophosphatemia; rickets.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
Similar articles
-
Rickets guidance: part II-management.Pediatr Nephrol. 2022 Oct;37(10):2289-2302. doi: 10.1007/s00467-022-05505-5. Epub 2022 Mar 29. Pediatr Nephrol. 2022. PMID: 35352187 Free PMC article.
-
Safety and efficacy of burosumab in improving phosphate metabolism, bone health, and quality of life in adolescents with X-linked hypophosphatemic rickets.Eur J Med Genet. 2024 Aug;70:104958. doi: 10.1016/j.ejmg.2024.104958. Epub 2024 Jun 29. Eur J Med Genet. 2024. PMID: 38950880
-
X-Linked Hypophosphatemia and FGF23-Related Hypophosphatemic Diseases: Prospect for New Treatment.Endocr Rev. 2018 Jun 1;39(3):274-291. doi: 10.1210/er.2017-00220. Endocr Rev. 2018. PMID: 29381780 Review.
-
Advances in understanding of phosphate homeostasis and related disorders.Endocr J. 2022 Aug 29;69(8):881-896. doi: 10.1507/endocrj.EJ22-0239. Epub 2022 Jul 13. Endocr J. 2022. PMID: 35831119 Review.
-
Diagnosis and management of X-linked hypophosphatemia in children and adolescent in the Gulf Cooperation Council countries.Arch Osteoporos. 2021 Mar 4;16(1):52. doi: 10.1007/s11657-021-00879-9. Arch Osteoporos. 2021. PMID: 33660084 Free PMC article.
Cited by
-
Lessons learned from the real-world diagnosis and management of hereditary hypophosphatemic rickets.Bone Rep. 2024 Mar 21;21:101753. doi: 10.1016/j.bonr.2024.101753. eCollection 2024 Jun. Bone Rep. 2024. PMID: 39011543 Free PMC article.
-
Etiology and Biochemical Profile of Rickets in Tertiary Care Centres in Eastern India: A Retrospective Cross-sectional Study.Indian J Endocrinol Metab. 2024 Mar-Apr;28(2):184-191. doi: 10.4103/ijem.ijem_221_23. Epub 2024 Apr 29. Indian J Endocrinol Metab. 2024. PMID: 38911108 Free PMC article.
-
Burosumab treatment of a child with McCune-Albright syndrome/polyostotic fibrous dysplasia: challenges and benefits.JBMR Plus. 2025 Mar 10;9(5):ziaf042. doi: 10.1093/jbmrpl/ziaf042. eCollection 2025 May. JBMR Plus. 2025. PMID: 40297189 Free PMC article.
-
Burosumab, a Transformational Treatment in a Pediatric Patient With Cutaneous-Skeletal Hypophosphatemia Syndrome.JCEM Case Rep. 2024 Oct 16;2(10):luae184. doi: 10.1210/jcemcr/luae184. eCollection 2024 Oct. JCEM Case Rep. 2024. PMID: 39416269 Free PMC article.
-
Approach to Rickets: Is It Calciopenic or Phosphopenic?Turk Arch Pediatr. 2023 Sep;58(5):458-466. doi: 10.5152/TurkArchPediatr.2023.23050. Turk Arch Pediatr. 2023. PMID: 37427438 Free PMC article.
References
-
- Mughal MZ. Rickets. Curr Osteoporos Rep. 2011;9(4):291–299. - PubMed
-
- Beck-Nielsen SS, Jensen TK, Gram J, Brixen K, Brock-Jacobsen B. Nutritional rickets in Denmark: a retrospective review of children’s medical records from 1985 to 2005. Eur J Pediatr. 2009;168(8):941–949. - PubMed
-
- Arenas MA, Jaimovich S, Perez Garrido N, et al. Hereditary hypophosphatemic rickets and craniosynostosis. J Pediatr Endocrinol Metab. 2021;34(9):1105–1113. - PubMed
-
- Lecoq AL, Brandi ML, Linglart A, Kamenický P. Management of X-linked hypophosphatemia in adults. Metab Clin Exp. 2020;103(s):154049. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
