

Medical cannabinoids: a pharmacology-based systematic review and meta-analysis for all relevant medical indications
- PMID: 35982439
- PMCID: PMC9389720
- DOI: 10.1186/s12916-022-02459-1
Medical cannabinoids: a pharmacology-based systematic review and meta-analysis for all relevant medical indications
Abstract
Background: Medical cannabinoids differ in their pharmacology and may have different treatment effects. We aimed to conduct a pharmacology-based systematic review (SR) and meta-analyses of medical cannabinoids for efficacy, retention and adverse events.
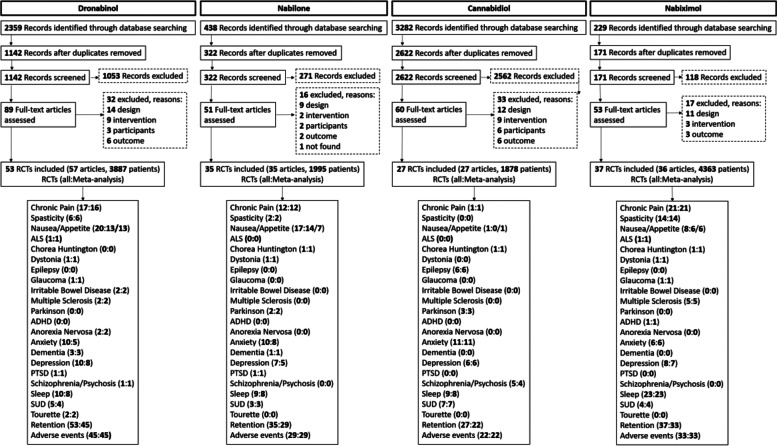
Methods: We systematically reviewed (registered at PROSPERO: CRD42021229932) eight databases for randomized controlled trials (RCTs) of dronabinol, nabilone, cannabidiol and nabiximols for chronic pain, spasticity, nausea /vomiting, appetite, ALS, irritable bowel syndrome, MS, Chorea Huntington, epilepsy, dystonia, Parkinsonism, glaucoma, ADHD, anorexia nervosa, anxiety, dementia, depression, schizophrenia, PTSD, sleeping disorders, SUD and Tourette. Main outcomes and measures included patient-relevant/disease-specific outcomes, retention and adverse events. Data were calculated as standardized mean difference (SMD) and ORs with confidence intervals (CI) via random effects. Evidence quality was assessed by the Cochrane Risk of Bias and GRADE tools.
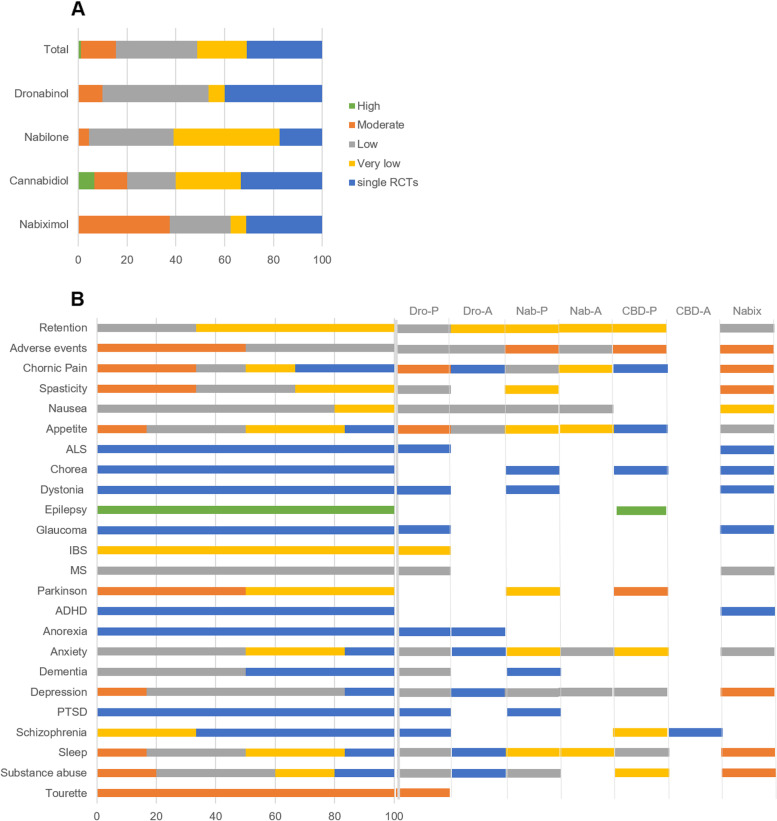
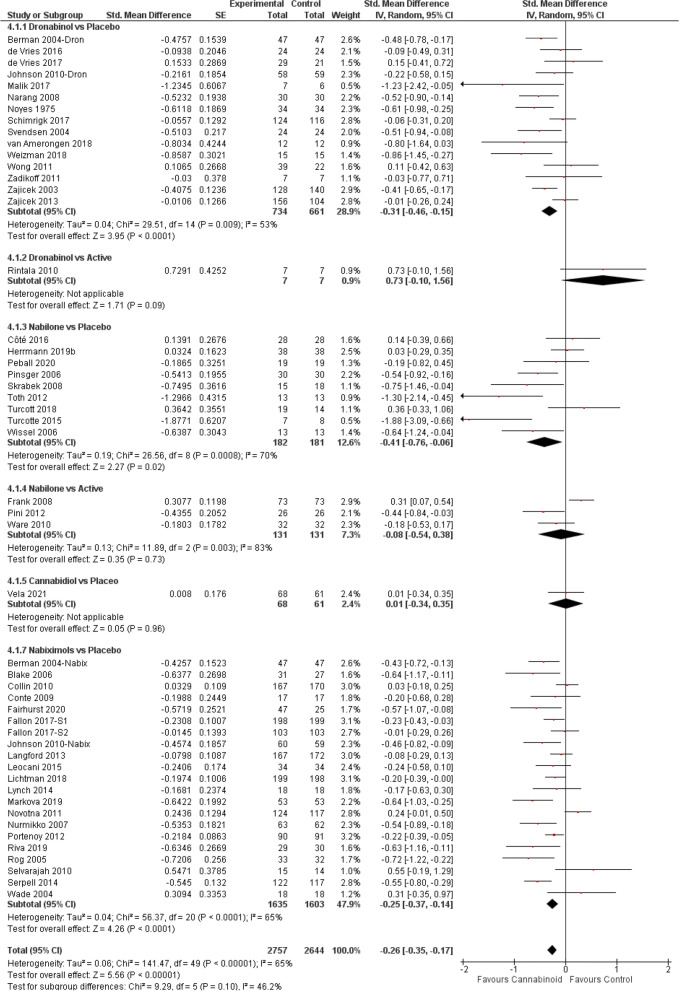
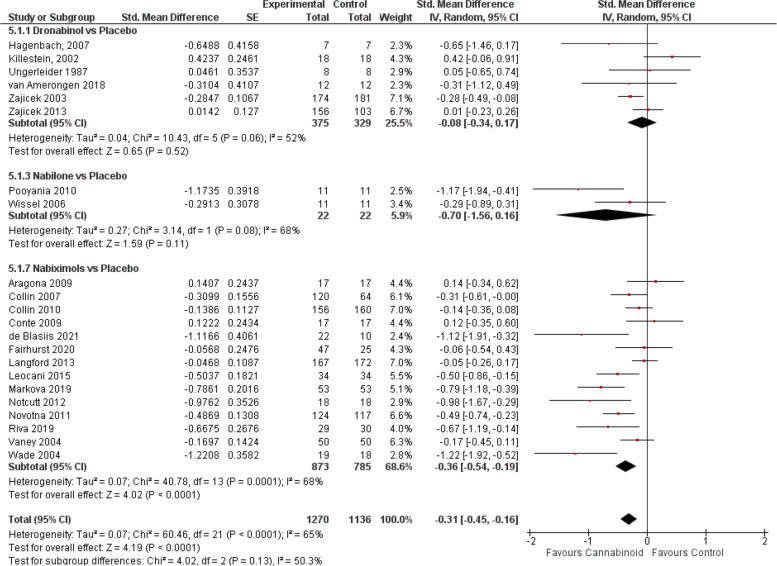
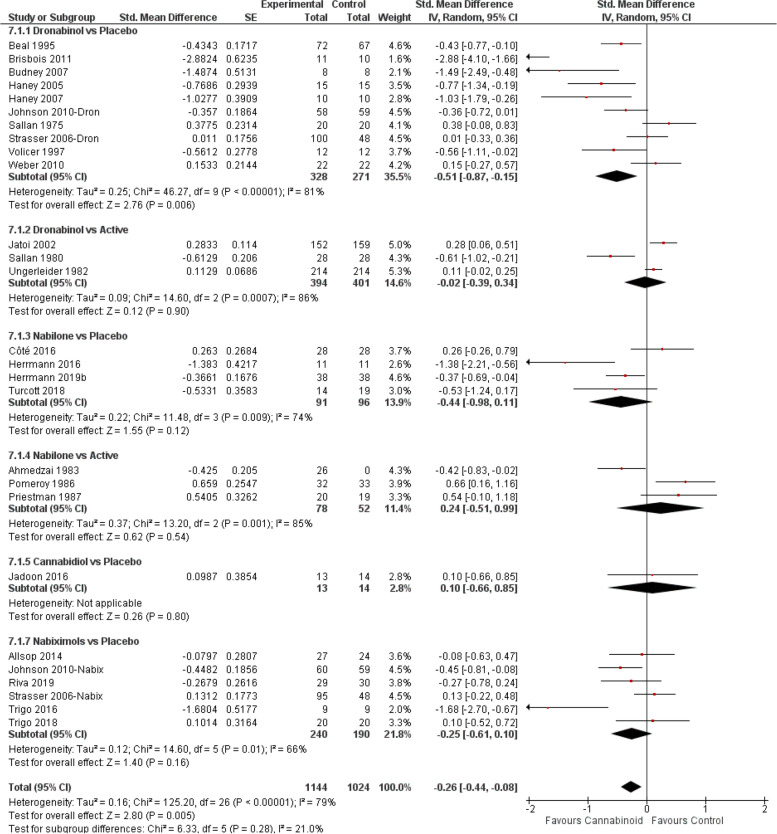
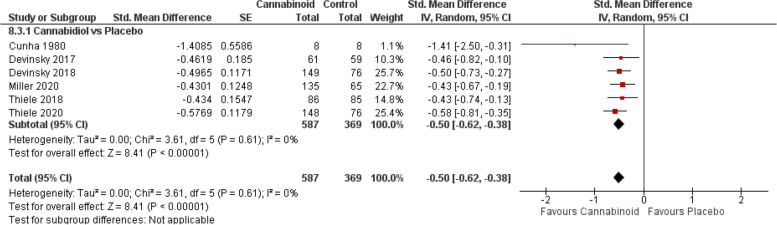
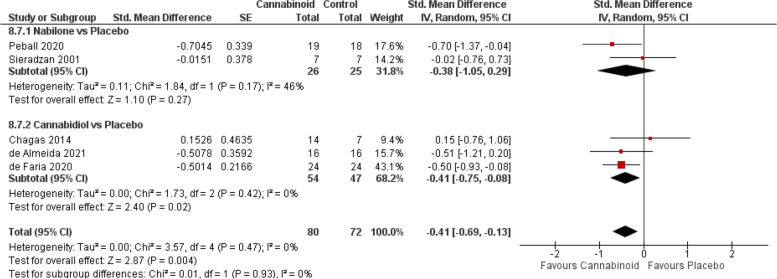
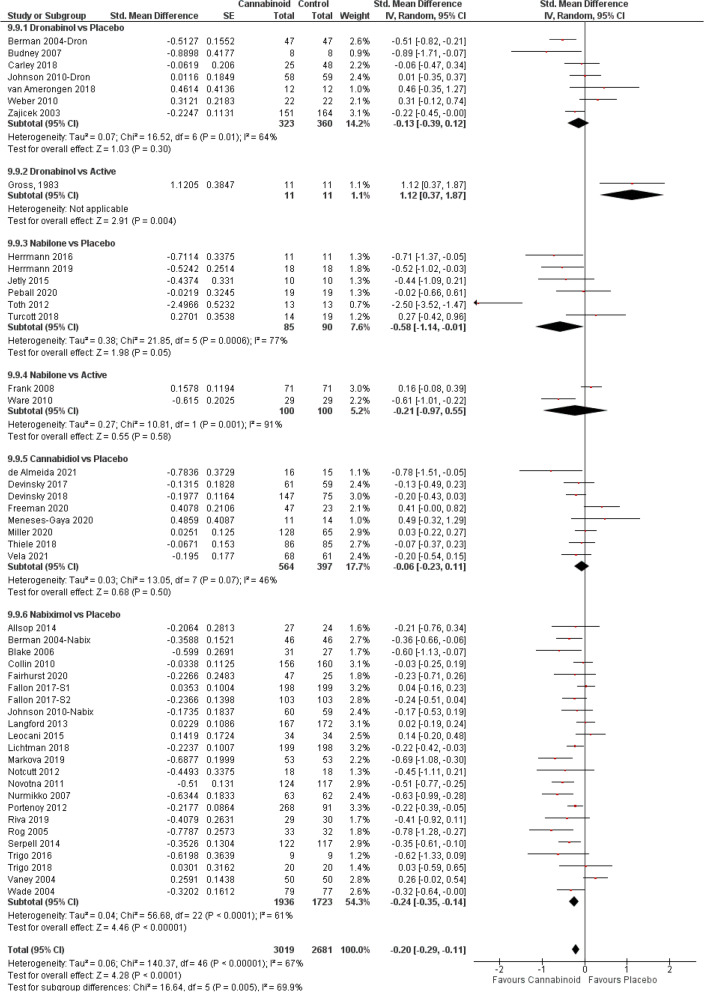
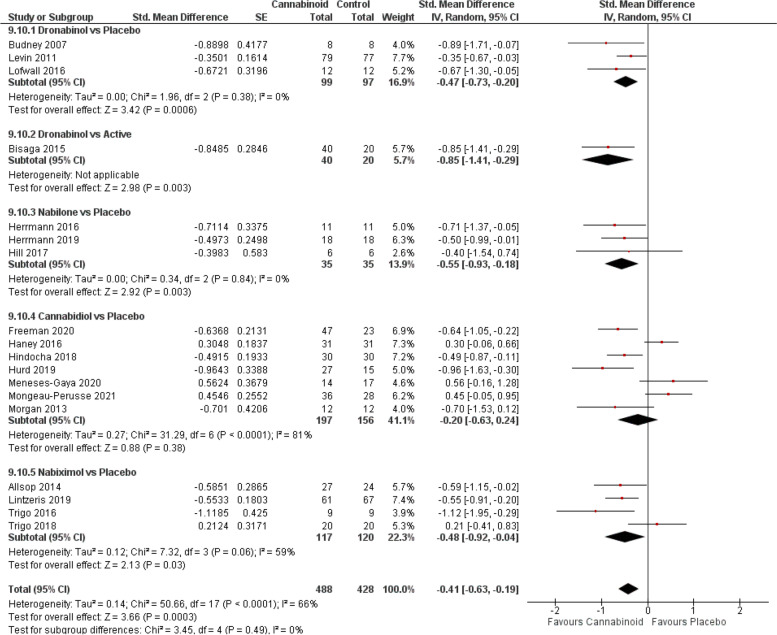
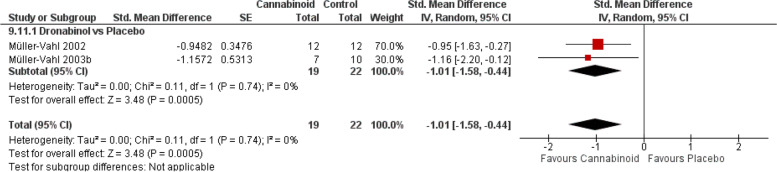
Results: In total, 152 RCTs (12,123 participants) were analysed according to the type of the cannabinoid, outcome and comparator used, resulting in 84 comparisons. Significant therapeutic effects of medical cannabinoids show a large variability in the grade of evidence that depends on the type of cannabinoid. CBD has a significant therapeutic effect for epilepsy (SMD - 0.5[CI - 0.62, - 0.38] high grade) and Parkinsonism (- 0.41[CI - 0.75, - 0.08] moderate grade). There is moderate evidence for dronabinol for chronic pain (- 0.31[CI - 0.46, - 0.15]), appetite (- 0.51[CI - 0.87, - 0.15]) and Tourette (- 1.01[CI - 1.58, - 0.44]) and moderate evidence for nabiximols on chronic pain (- 0.25[- 0.37, - 0.14]), spasticity (- 0.36[CI - 0.54, - 0.19]), sleep (- 0.24[CI - 0.35, - 0.14]) and SUDs (- 0.48[CI - 0.92, - 0.04]). All other significant therapeutic effects have either low, very low, or even no grade of evidence. Cannabinoids produce different adverse events, and there is low to moderate grade of evidence for this conclusion depending on the type of cannabinoid.
Conclusions: Cannabinoids are effective therapeutics for several medical indications if their specific pharmacological properties are considered. We suggest that future systematic studies in the cannabinoid field should be based upon their specific pharmacology.
Keywords: Adverse events; Cannabinoids; Clinical trial; Efficacy; Medical conditions; Neuropsychiatry; Pharmacology.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Ben AM. Cannabinoids in medicine: a review of their therapeutic potential. J Ethnopharmacol. 2006;105(1–2):1–25. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
