

Declining Prevalence of Human Immunodeficiency Virus (HIV)-Associated Neurocognitive Disorders in Recent Years and Associated Factors in a Large Cohort of Antiretroviral Therapy-Treated Individuals With HIV
- PMID: 35982541
- PMCID: PMC9907497
- DOI: 10.1093/cid/ciac658
Declining Prevalence of Human Immunodeficiency Virus (HIV)-Associated Neurocognitive Disorders in Recent Years and Associated Factors in a Large Cohort of Antiretroviral Therapy-Treated Individuals With HIV
Abstract
Background: HIV-associated neurocognitive disorders (HAND) have been suggested as persistent even with effective antiretroviral therapy (ART). Aims were to evaluate HAND prevalence and associated factors, in a large cohort of people-with-HIV (PWH).
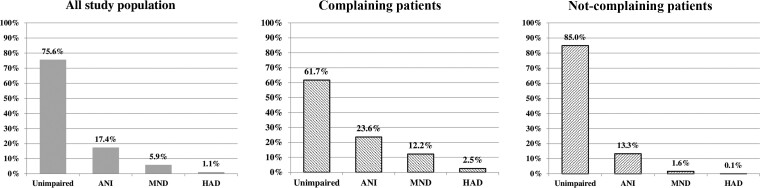
Methods: ART-treated PWH, underwent a neuropsychological examination through a battery of 12 tests exploring 5 different domains, between 2009 and 2020, were included in this cross-sectional analysis. HAND were classified according to Frascati's criteria. Participants were defined as complaining or not-complaining if a cognitive complaint was reported or not. Chi-square for trend and multivariable logistic regression were fitted.
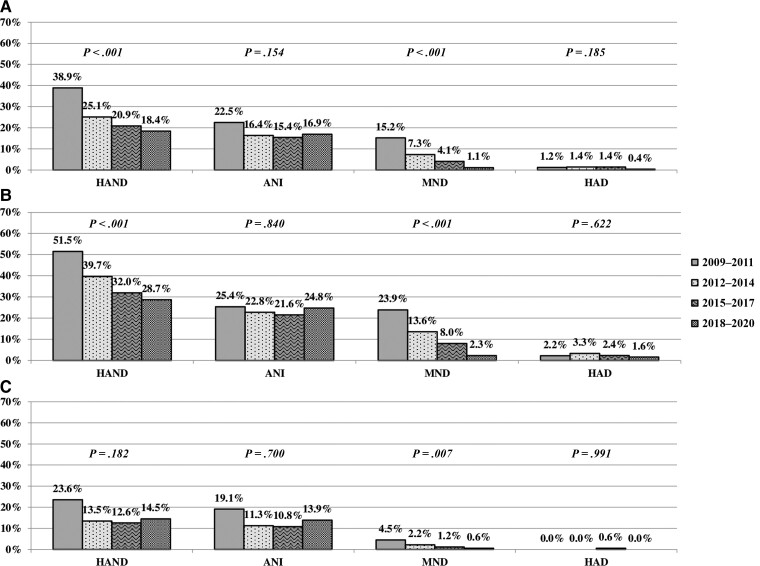
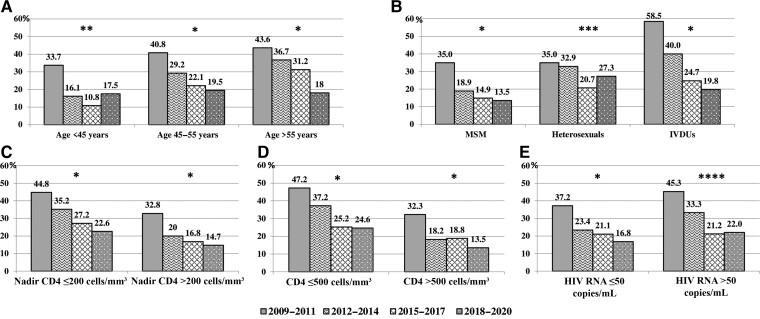
Results: Overall, 1424 PWH were enrolled during four three-years periods. HAND prevalence was 24%; among complainers (572/1424), it was 38%, higher than among not-complainers (15%). Over the study period, a decreasing HAND prevalence was found in the entire population (P < 0.001) and in complaining (P < 0.001); in not-complaining it remained stable (P = 0.182). Factors associated with HAND were older age, lower educational level, lower current CD4+ T-cell count and HCV co-infection. Compared to nonnucleoside reverse transcriptase inhibitors, receiving dual and integrase strand transfer inhibitor (INSTI)-based therapies was associated with a decreased risk of HAND, as well as being tested in more recent years.
Conclusions: In this large cohort of ART-treated PWH, mostly virologically suppressed, a remarkable decreasing HAND prevalence was observed. Besides HIV- and patient-related factors, the reduced risk of HAND found with dual and INSTI-based regimens along with a more recent ART initiation, could suggest a potential role of new treatment strategies in this decline, due to their greater virologic efficacy and better tolerability.
Keywords: AIDS; HIV; HIV-associated neurocognitive disorders (HAND); integrase strand transfer inhibitor; neurocognitive impairment.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. Andrea Antinori has served as a paid consultant to and received payment or honoraria from Astra-Zeneca, Gilead Sciences, GlaxoSmithKline, Janssen-Cilag, Merck Sharp and Dohme, Roche, Theratotecnologies, ViiV Healthcare. Rita Bellagamba reports payment or honoraria from Merck Sharp and Dohme, and participation on a Data Safety Monitoring Board or Advisory Board from ViiV Healthcare, Gilead Sciences, and Merck Sharp and Dohme. Marta Camici received institutional grant and support for attending meetings and/or travel from Gilead Sciences. Stefania Cicalini reports consulting fees paid to self from ViiV Healthcare, Jansen-Cilag, Merck Sharp and Dohme, Gilead Sciences; payment or honoraria from ViiV Healthcare, Jansen-Cilag, Merck Sharp and Dohme, and Gilead Sciences. Roberta Gagliardini reports payments to their institution from Gilead Sciences, speakers' honoraria/educational activities for ViiV Healthcare, Merck Sharp and Dohme and Gilead Sciences, support for attending meetings and/or travel from ViiV Healthcare, advisor for Theratechnologies, Janssen-Cilag and Gilead Sciences. Ilaria Mastrorosa received institutional grant and support for attending meetings and/or travel from Gilead Sciences. Carmela Pinnetti received personal fee from Gilead Sciences for a case presentation and a travel grant and served on an advisory board for Janssen-Cilag. Alessandra Vergori received institutional grant from Gilead Sciences, speakers' honoraria/educational activities for Merck Sharp and Dohme and Janssen-Cilag, advisor for Janssen-Cilag. The other co-authors declare no conflicts of interests.
Figures
References
-
- Winston A, Spudich S. Cognitive disorders in people living with HIV. Lancet HIV 2020; 7:e504–13. - PubMed
-
- Bhaskaran K, Mussini C, Antinori A, et al. Changes in the incidence and predictors of human immunodeficiency virus associated dementia in the era of highly active antiretroviral therapy. Ann Neurol 2008; 63:213–21. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
