

Open Globe Injuries: Review of Evaluation, Management, and Surgical Pearls
- PMID: 35983163
- PMCID: PMC9379121
- DOI: 10.2147/OPTH.S372011
Open Globe Injuries: Review of Evaluation, Management, and Surgical Pearls
Abstract
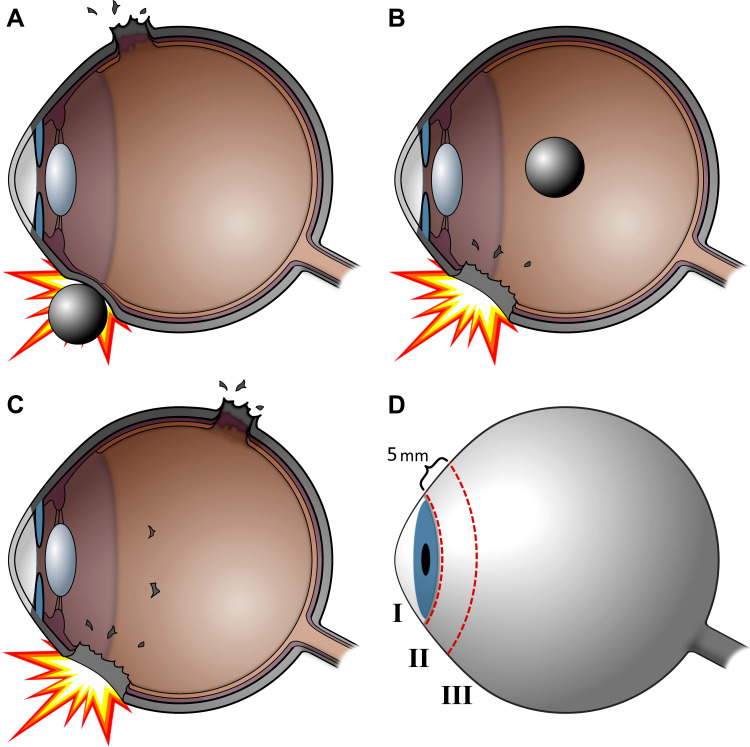
Ocular trauma may either be closed globe or open globe. Open globe injuries are full-thickness defects of the eyewall and are often differentiated by the mechanisms of injury from which they are caused: sharp or blunt trauma. They are ocular emergencies and can lead to substantial visual morbidity. Without timely intervention, damage is irreversible and leads to permanent vision loss. The goals of evaluation are to identify the mechanism of injury, characterize the extent of injury, and gather relevant history. If an open globe is suspected, ophthalmologic consultation should be requested. Once an open globe is diagnosed, preparations for surgery should be made immediately and steps should be taken to avoid further injury. Intraocular infection risk is relatively high, requiring immediate empiric systemic antibiotics. Emergent surgical exploration and primary closure is indicated whenever possible. After initial closure, secondary surgery and revision may be needed to improve vision outcomes, followed by extensive follow-up. In this review, best practices for evaluation and management are reviewed, with particular focus on the surgical approach and techniques.
Keywords: ocular trauma; open globe surgery; open globe surgical pearls; ophthalmic surgery; repair of open globe.
© 2022 Zhou et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures





References
-
- Kolb H. Gross Anatomy of the Eye. Salt Lake City (UT): University of Utah Health Sciences Center; 1995. - PubMed
-
- Duke-Elder SMPA. System of Ophthalmology Vol. 14, Part 1. London: KimptonSt. Louis: Mosby; 1972.
-
- Kuhn F, Pelayes DE. Management of the ruptured eye. Eur Ophth Rev. 2009;3(1):48–50. doi:10.17925/EOR.2009.03.01.48 - DOI
Publication types
LinkOut - more resources
Full Text Sources
