

Development and external validation of DISPAIR fistula risk score for clinically relevant postoperative pancreatic fistula risk after distal pancreatectomy
- PMID: 35983583
- PMCID: PMC10364701
- DOI: 10.1093/bjs/znac266
Development and external validation of DISPAIR fistula risk score for clinically relevant postoperative pancreatic fistula risk after distal pancreatectomy
Abstract
Background: Highly utilized risk scores for clinically relevant postoperative pancreatic fistula (CR-POPF) have guided clinical decision-making in pancreatoduodenectomy. However, none has been successfully developed for distal pancreatectomy. This study aimed to develop and validate a new fistula risk score for distal pancreatectomy.
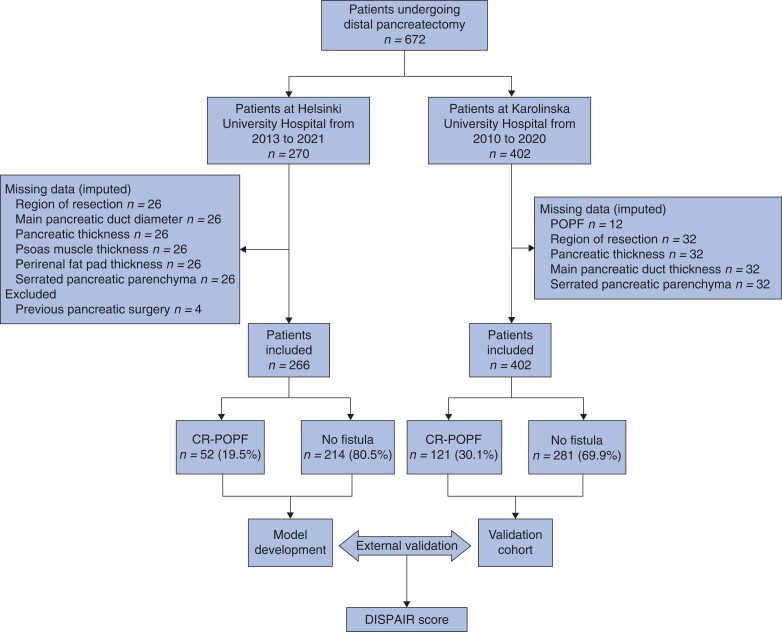
Methods: Patients undergoing distal pancreatectomy at Helsinki University Hospital, Finland from 2013 to 2021, and at Karolinska University Hospital, Sweden, from 2010 to 2020, were included retrospectively. The outcome was CR-POPF, according to the 2016 International Study Group of Pancreatic Surgery definition. Preoperative clinical demographics and radiological parameters such as pancreatic thickness and duct diameter were measured. A logistic regression model was developed, internally validated with bootstrapping, and the performance assessed in an external validation cohort.
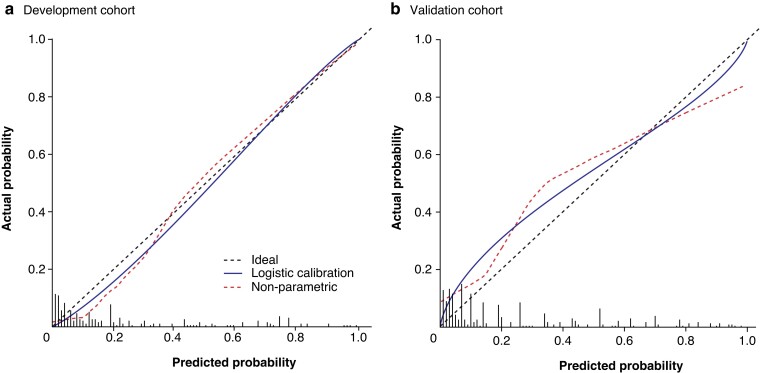
Results: Of 668 patients from Helsinki (266) and Stockholm (402), 173 (25.9 per cent) developed CR-POPF. The final model consisted of three variables assessed before surgery: transection site (neck versus body/tail), pancreatic thickness at transection site, and diabetes. The model had an area under the receiver operating characteristic curve (AUROC) of 0.904 (95 per cent c.i. 0.855 to 0.949) after internal validation, and 0.798 (0.748 to 0.848) after external validation. The calibration slope and intercept on external validation were 0.719 and 0.192 respectively. Four risk groups were defined in the validation cohort for clinical applicability: low (below 5 per cent), moderate (at least 5 but below 30 per cent), high (at least 30 but below 75 per cent), and extreme (75 per cent or more). The incidences in these groups were 8.7 per cent (11 of 126), 22.0 per cent (36 of 164), 63 per cent (57 of 91), and 81 per cent (17 of 21) respectively.
Conclusion: The DISPAIR score after distal pancreatectomy may guide decision-making and allow a risk-adjusted outcome comparison for CR-POPF.
© The Author(s) 2022. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures
References
-
- Miao Y, Lu Z, Yeo CJ, Vollmer CM, Fernandez-del Castillo C, Ghaneh P et al. Management of the pancreatic transection plane after left (distal) pancreatectomy: expert consensus guidelines by the international study group of pancreatic surgery (ISGPS). Surgery 2020;168:72–84 - PubMed
-
- McMillan MT, Christein JD, Callery MP, Behrman SW, Drebin JA, Hollis RH et al. Comparing the burden of pancreatic fistulas after pancreatoduodenectomy and distal pancreatectomy. Surgery 2016;159:1013–1022. - PubMed
-
- Callery MP, Pratt WB, Kent TS, Chaikof EL, Vollmer CM. A prospectively validated clinical risk score accurately predicts pancreatic fistula after pancreatoduodenectomy. J Am Coll Surg 2013;216:1–14 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
