

Hemoperfusion in the intensive care unit
- PMID: 35984473
- PMCID: PMC9389493
- DOI: 10.1007/s00134-022-06810-1
Hemoperfusion in the intensive care unit
Abstract
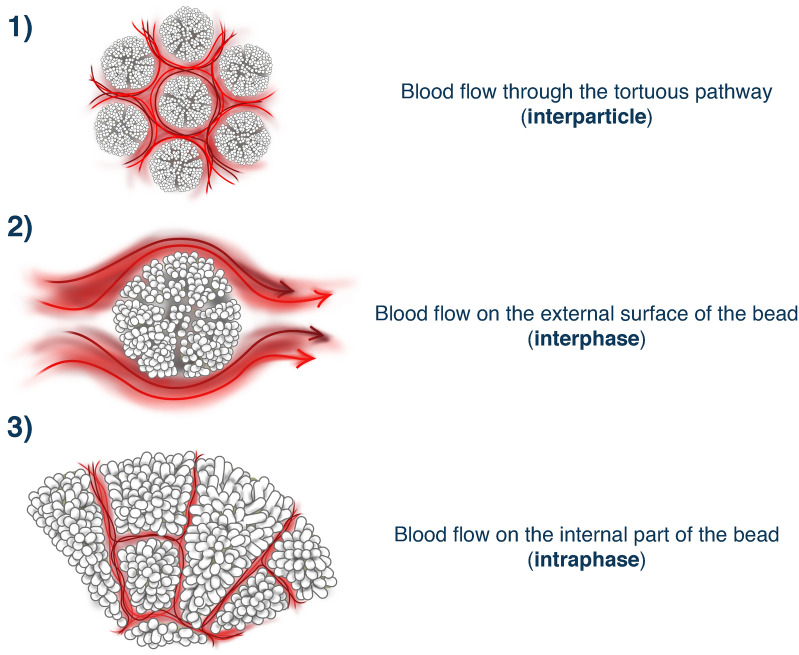
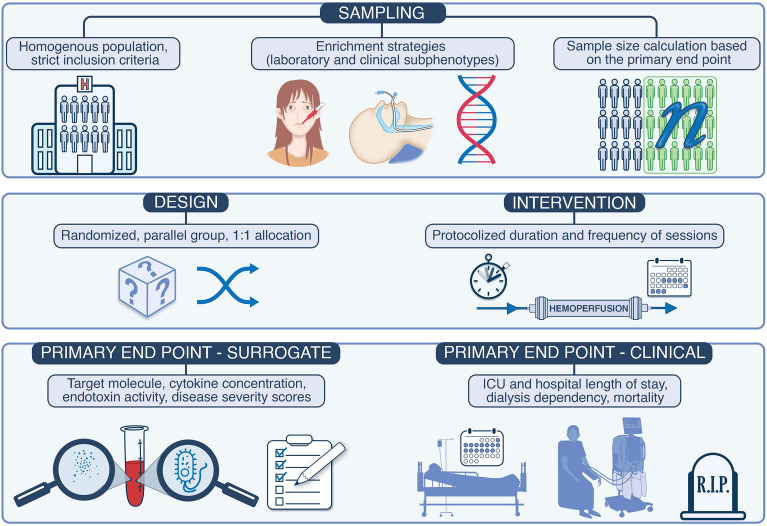
Multiple organ failure following a septic event derives from immune dysregulation. Many of the mediators of this process are humoral factors (cytokines), which could theoretically be cleared by direct adsorption through a process called hemoperfusion. Hemoperfusion through devices, which bind specific molecules like endotoxin or theoretically provide non-specific adsorption of pro-inflammatory mediators has been attempted and studied for several decades with variable results. More recently, technological evolution has led to the increasing application of adsorption due to more biocompatible and possibly more efficient biomaterials. As a result, new indications are developing in this field, and novel tools are available for clinical use. This narrative review will describe current knowledge regarding technical concepts, safety, and clinical results of hemoperfusion. Finally, it will focus on the most recent literature regarding adsorption applied in critically ill patients and their indications, including recent randomized controlled trials and future areas of investigation. Clinical trials for the assessment of efficacy of hemoperfusion in septic patients should apply the explanatory approach. This includes a highly selected homogenous patient population. Enrichment criteria such as applying genetic signature and molecular biomarkers allows the identification of subphenotypes of patients. The intervention must be delivered by a multidisciplinary team of trained personnel. The aim is to maximize the signals for efficacy and safety. In a homogenous cohort, confounding uncontrolled variables are less likely to exist. Trials with highly selected populations have a high internal validity but poor generalizability. The parallel design described in the figure is robust and usually is required by regulatory agencies for the approval of a new treatment. Allocation concealment and randomization are key to minimize bias such as confirmation bias, observer bias. The intervention should be delivered following a strict protocol. Deviations from the protocol might negatively influence the potential effects of the therapies. Surrogates such as cytokine measurement are adequate primary outcomes in phase 3 trials with small sample size because there is a higher likelihood of finding positive results concerning surrogate markers than in respect with clinical outcomes. Once a trial shows positive results concerning surrogate markers, a rationale for another phase 3 trial exploring clinical outcomes is built, justifying the allocation of financial sources to the intended trial.
Keywords: Adsorption; Blood purification; COVID-19; Cytokine; Hemoperfusion; Lipopolysaccharide; Sepsis.
© 2022. The Author(s).
Conflict of interest statement
ZR declares he received grants from BBraun. SR declares he received grants from Baxter an BBraun. TR has received funding for lectures, and been consultant or advisory board member for AstraZeneca, BBraun, Baxter, bioMérieux, Contatti Medical (CytoSorbents), Eurofarma, Jafron, Life Pharma, and Nova Biomedical. RB has received unrestricted research grants to investigate drug clearance with hemoperfusion and payment for advisory committee work by Jafron Biomedical Co Ltd. CR has been receiving honoraria, grants for studies or has been part of the advisory board and speaker bureau of the following companies in the last 3 years: Astute medical, Aferetica, Astrazeneca, Asahi Medical, Biomerieux, Baxter, Cytosorbents, Fresenius Medical Care, GE, ESTOR, Jafron, Medica, Medtronic, Novartis, Toray.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
