

Mortality Patterns of Synchronous Uterine and Ovarian Cancers: A SEER Registry Analysis
- PMID: 35984988
- PMCID: PMC9633557
- DOI: 10.1158/1055-9965.EPI-22-0587
Mortality Patterns of Synchronous Uterine and Ovarian Cancers: A SEER Registry Analysis
Abstract
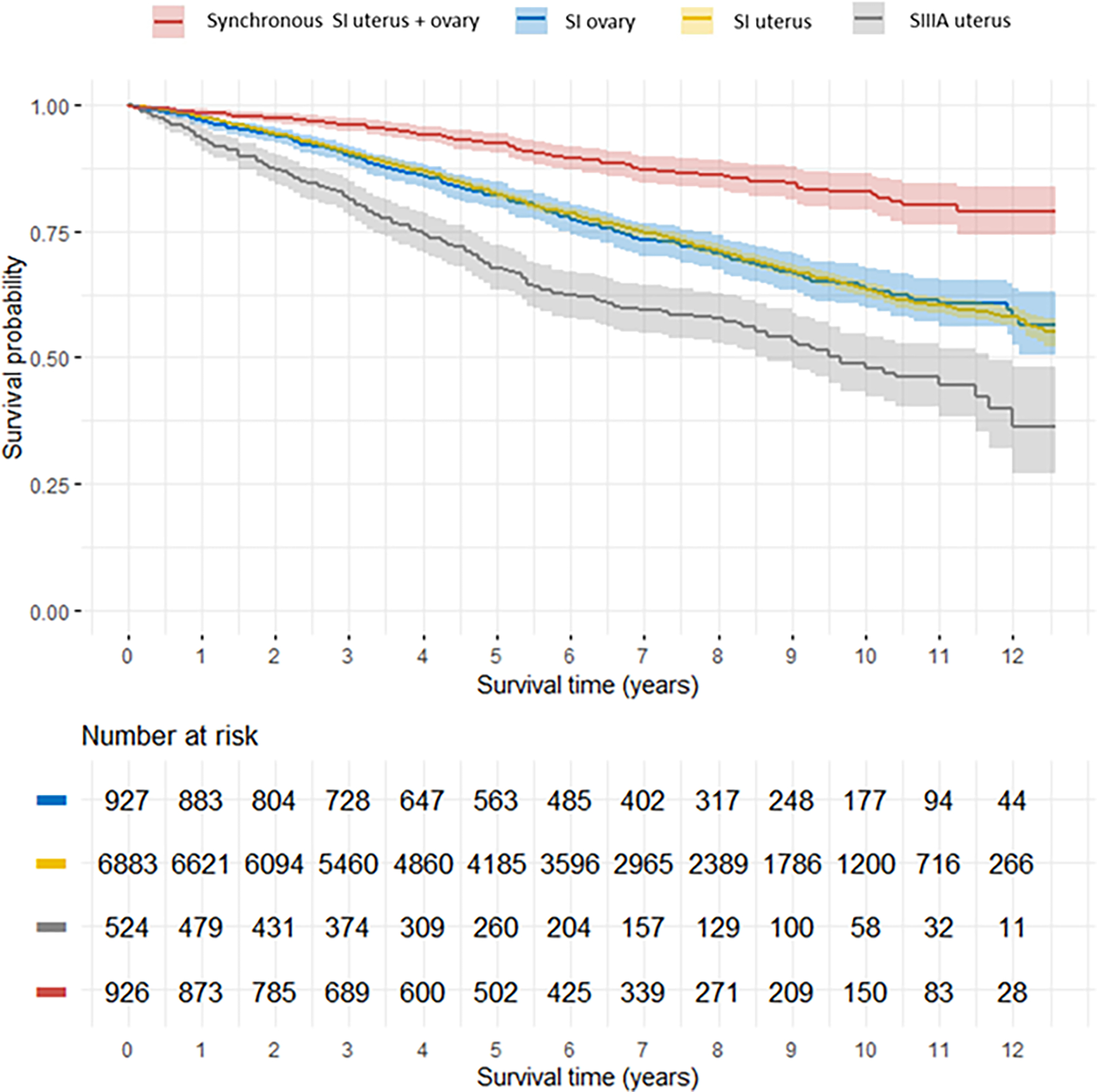
Background: The degree to which uterine cancer metastatic to the ovary is misdiagnosed as synchronous stage I uterine and ovarian cancers is unclear. We sought to determine whether patients with synchronous cancers had mortality patterns similar to either stage IIIA uterine, stage I uterine, or stage I ovarian cancers alone.
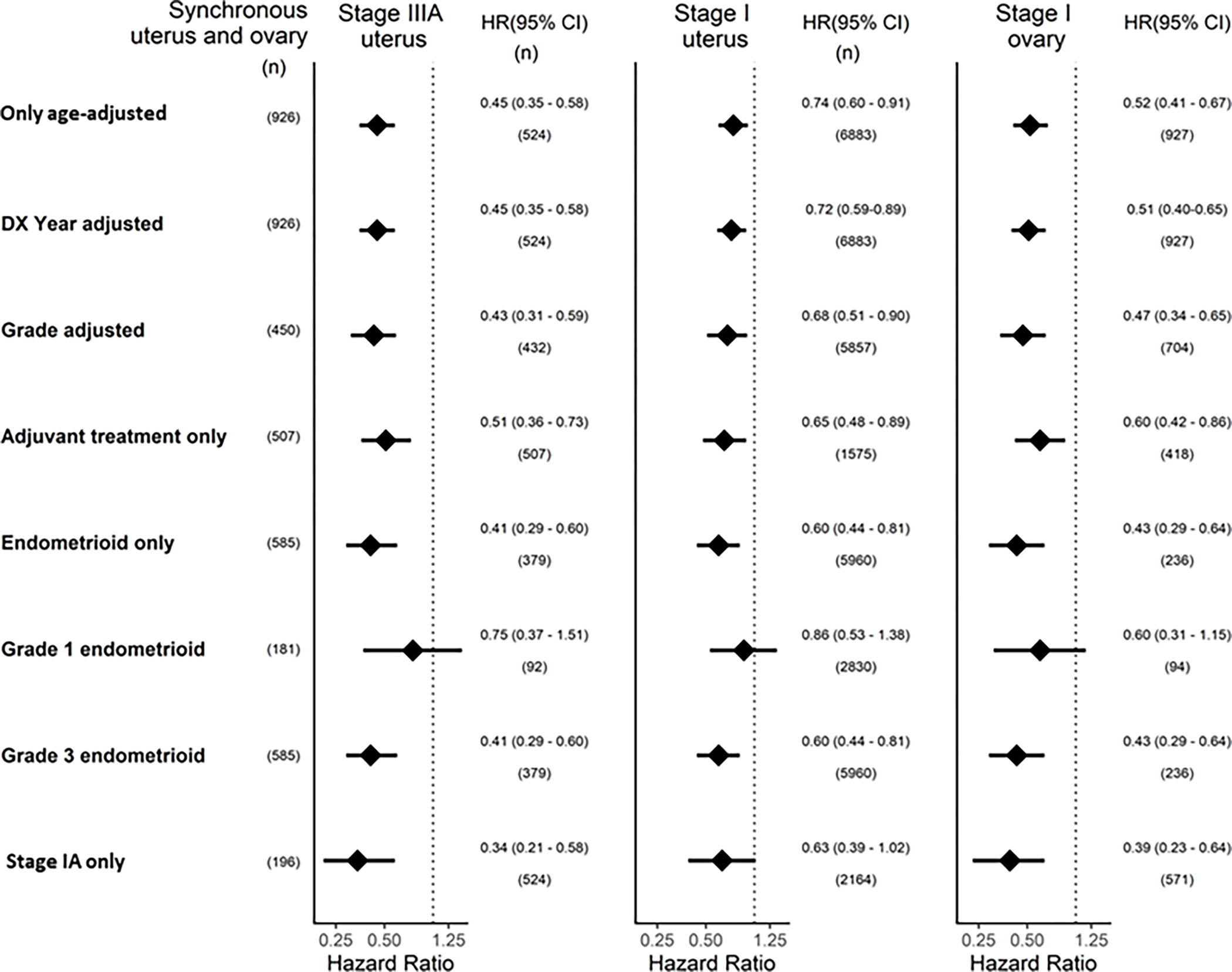
Methods: The Surveillance, Epidemiology, and End Results database was used to compare mortality of patients with synchronous stage I uterine and stage I ovarian cancers versus those with stage IIIA uterine, stage I uterine, or stage I ovarian cancers alone. We calculated age-adjusted mortality hazard ratios (HR) and 95% confidence intervals (CI) accounting for calendar year and grade, adjuvant treatment, grade 1 endometrioid cancers, grade 3 endometrioid cancers, and stage IA cancers.
Results: Among the 9,321 patients, we observed lower age-adjusted mortality in patients with stage I synchronous cancers (n = 937) compared to those with stage IIIA uterine (n = 531; HR, 0.45 95% CI, 0.35-0.58), stage I uterine (n = 6,919; HR, 0.74; 95% CI, 0.60-0.91), and stage I ovarian cancers (n = 934; HR, 0.52; 95% CI, 0.41-0.67). Results were similar after taking into account diagnosis year and grade, and limiting to those receiving adjuvant therapy, grade 1 or grade 3 endometrioid cancers, or stage IA cancers.
Conclusions: We observed lower mortality for synchronous stage I uterine and ovarian cancers, which was not explained by younger age, earlier stage, lower grade, histology type, or adjuvant therapy.
Impact: The possible misdiagnosis associated with clinicopathologic of synchronous uterine and ovarian cancers does not appear to worsen survival on a population level.
©2022 American Association for Cancer Research.
Conflict of interest statement
The authors report no conflict of interest
Figures
References
-
- Jamison PM, Altekruse SF, Chang JT, Zahn J, Lee R, Noone AM, et al. Site-Specific factors for cancer of the corpus uteri from seer registries: Collaborative stage data collection system, version 1 and version 2. Cancer [Internet]. 2014. Dec 1 [cited 2021 Jul 5];120(S23):3836–45. Available from: https://pubmed.ncbi.nlm.nih.gov/25412395/ - PubMed
-
- Soliman PT, Slomovitz BM, Broaddus RR, Sun CC, Oh JC, Eifel PJ, et al. Synchronous primary cancers of the endometrium and ovary: A single institution review of 84 cases. Gynecologic Oncology. 2004. Aug 1;94(2):456–62. - PubMed
-
- Oranratanaphan S, Manchana T, Sirisabya N. Clinicopathologic variables and survival comparison of patients with synchronous endometrial and ovarian cancers versus primary endometrial cancer with ovarian metastasis. Asian Pacific Journal of Cancer Prevention. 2008;9(3):403–8. - PubMed
-
- Bandera E v., Williams MG, Demissie K, Rodríguez-Rodríguez L. Synchronous primary ovarian and endometrial cancers: A population-based assessment of survival. Obstetrics and Gynecology [Internet]. 2009. Apr [cited 2021 Jul 5];113(4):783–9. Available from: https://pubmed.ncbi.nlm.nih.gov/19305320/ - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
