

Spontaneous subarachnoid haemorrhage
- PMID: 35985353
- PMCID: PMC9987649
- DOI: 10.1016/S0140-6736(22)00938-2
Spontaneous subarachnoid haemorrhage
Abstract
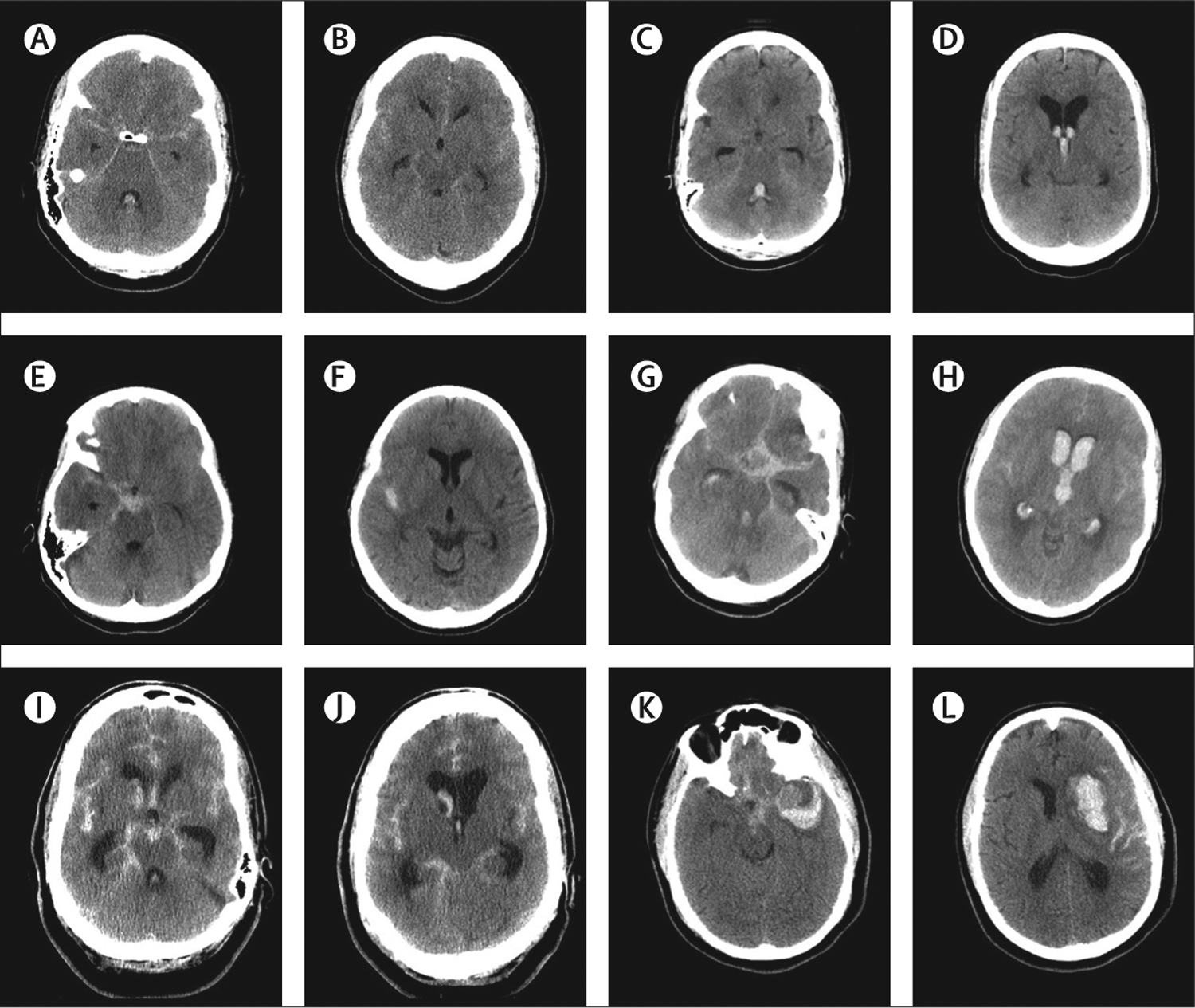
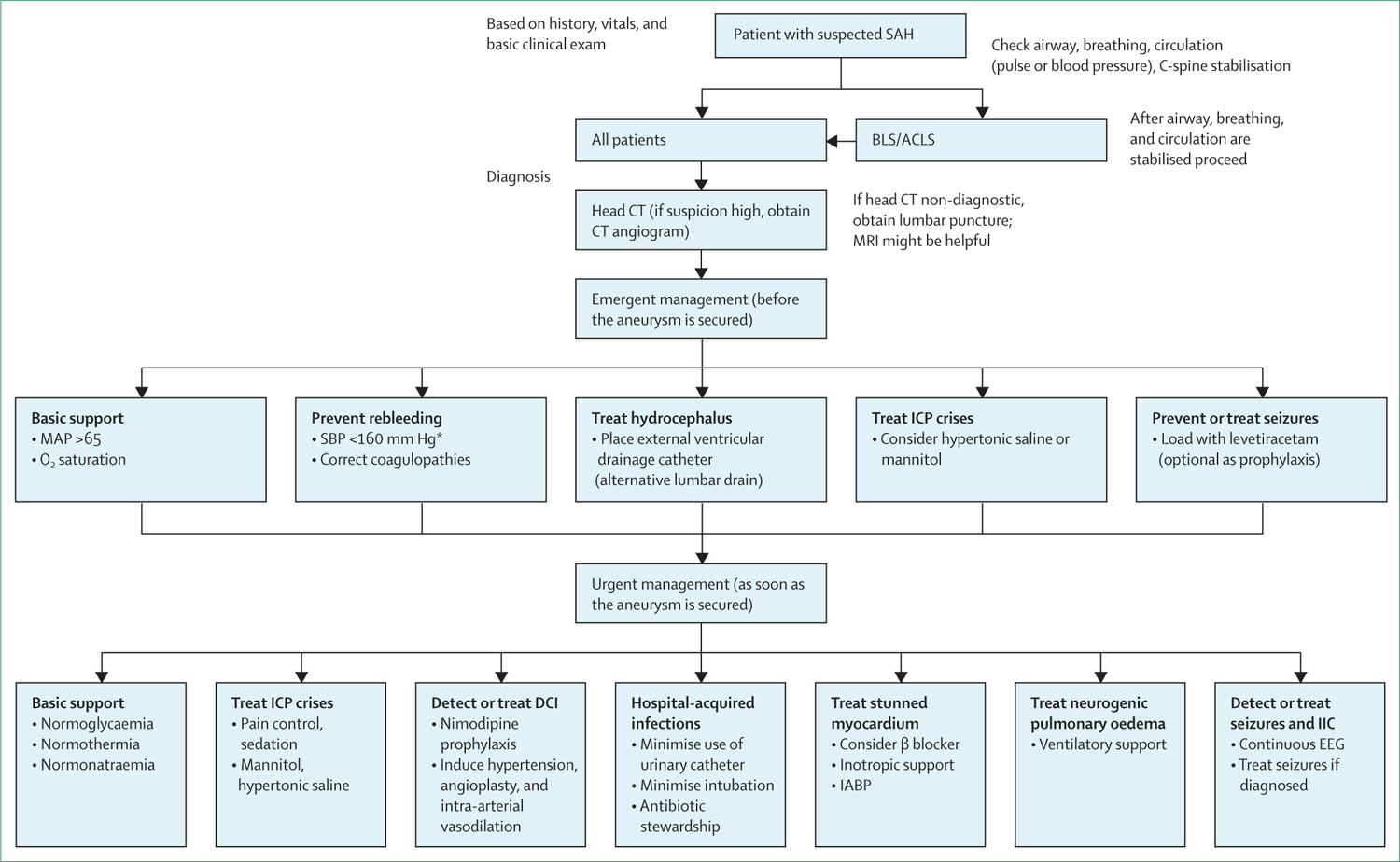
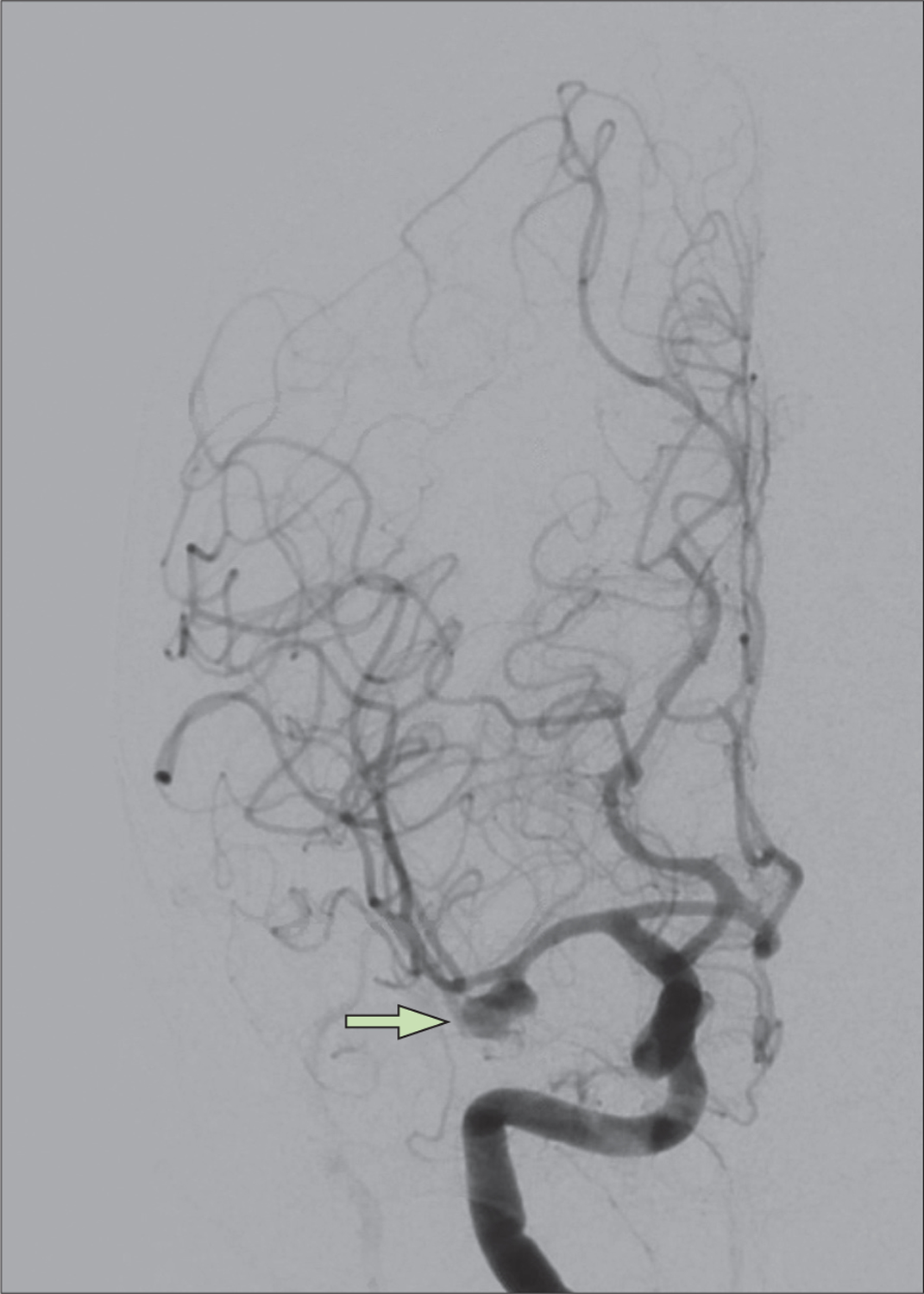
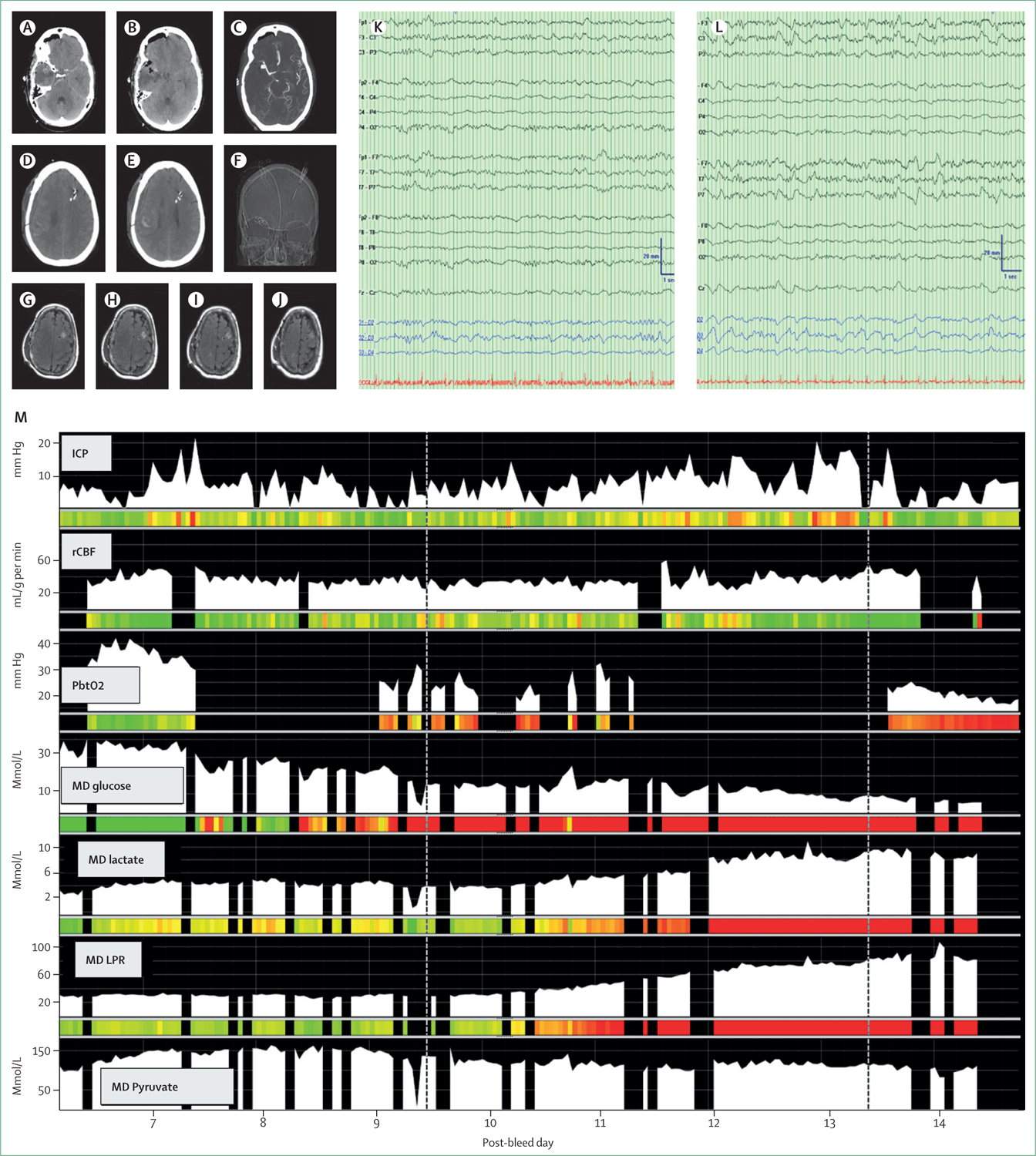
Subarachnoid haemorrhage (SAH) is the third most common subtype of stroke. Incidence has decreased over past decades, possibly in part related to lifestyle changes such as smoking cessation and management of hypertension. Approximately a quarter of patients with SAH die before hospital admission; overall outcomes are improved in those admitted to hospital, but with elevated risk of long-term neuropsychiatric sequelae such as depression. The disease continues to have a major public health impact as the mean age of onset is in the mid-fifties, leading to many years of reduced quality of life. The clinical presentation varies, but severe, sudden onset of headache is the most common symptom, variably associated with meningismus, transient or prolonged unconsciousness, and focal neurological deficits including cranial nerve palsies and paresis. Diagnosis is made by CT scan of the head possibly followed by lumbar puncture. Aneurysms are commonly the underlying vascular cause of spontaneous SAH and are diagnosed by angiography. Emergent therapeutic interventions are focused on decreasing the risk of rebleeding (ie, preventing hypertension and correcting coagulopathies) and, most crucially, early aneurysm treatment using coil embolisation or clipping. Management of the disease is best delivered in specialised intensive care units and high-volume centres by a multidisciplinary team. Increasingly, early brain injury presenting as global cerebral oedema is recognised as a potential treatment target but, currently, disease management is largely focused on addressing secondary complications such as hydrocephalus, delayed cerebral ischaemia related to microvascular dysfunction and large vessel vasospasm, and medical complications such as stunned myocardium and hospital acquired infections.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests JC is a minority shareholder at iCE Neurosystems. JC is supported by grant funding from the US National Institutes of Health (NIH; NS106014, NS112760) and the McDonnell Foundation. SP is supported by grant funding from the NIH (NS113055).
Figures
Comment in
-
Convexity subarachnoid haemorrhage.Lancet. 2023 Jan 21;401(10372):193-194. doi: 10.1016/S0140-6736(23)00004-1. Lancet. 2023. PMID: 36681413 No abstract available.
References
-
- Feigin VL, Lawes CM, Bennett DA, Barker-Collo SL, Parag V. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: a systematic review. Lancet Neurol 2009; 8: 355–69. - PubMed
-
- Etminan N, Rinkel GJ. Unruptured intracranial aneurysms: development, rupture and preventive management. Nat Rev Neurol 2016; 12: 699–713. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
