

Stereotactic Ablative Radiation for Systemic Therapy-naïve Oligometastatic Kidney Cancer
- PMID: 35985982
- PMCID: PMC9988242
- DOI: 10.1016/j.euo.2022.06.008
Stereotactic Ablative Radiation for Systemic Therapy-naïve Oligometastatic Kidney Cancer
Abstract
Background: Evidence-based guidelines for the management of systemic therapy-naïve oligometastatic renal cell carcinoma (RCC) are lacking.
Objective: To evaluate the potential of stereotactic ablative radiotherapy (SAbR) to provide longitudinal disease control while preserving quality of life (QOL) in patients with systemic therapy-naïve oligometastatic RCC.
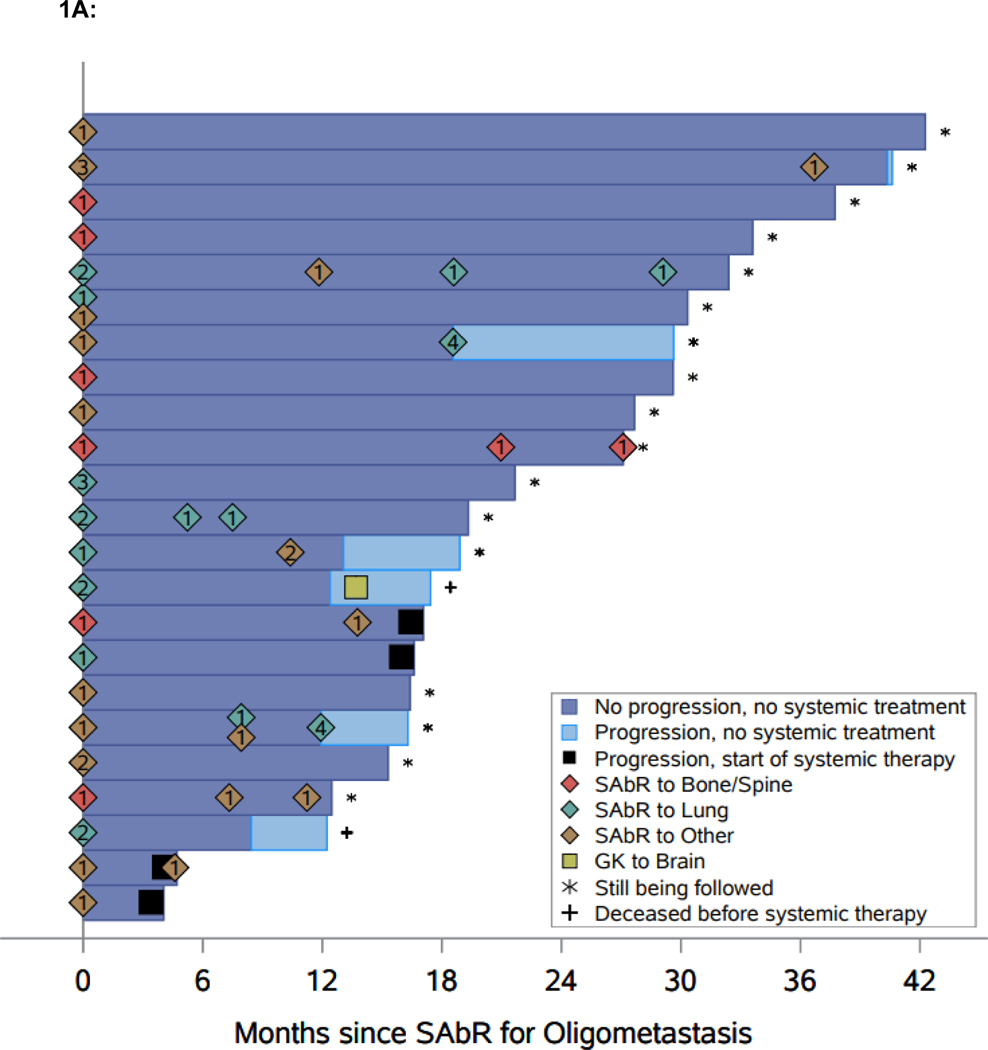
Design, setting, and participants: RCC patients with three or fewer extracranial metastases were eligible. SAbR was administered longitudinally to all upfront and, as applicable, subsequent metastases.
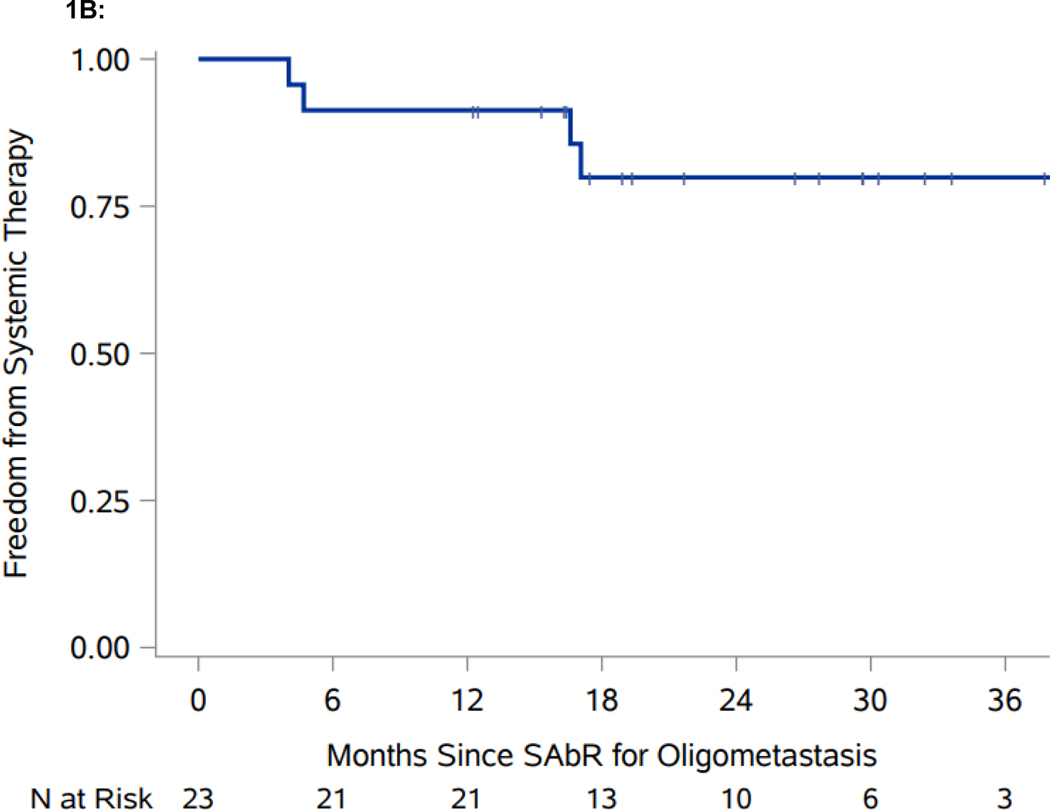
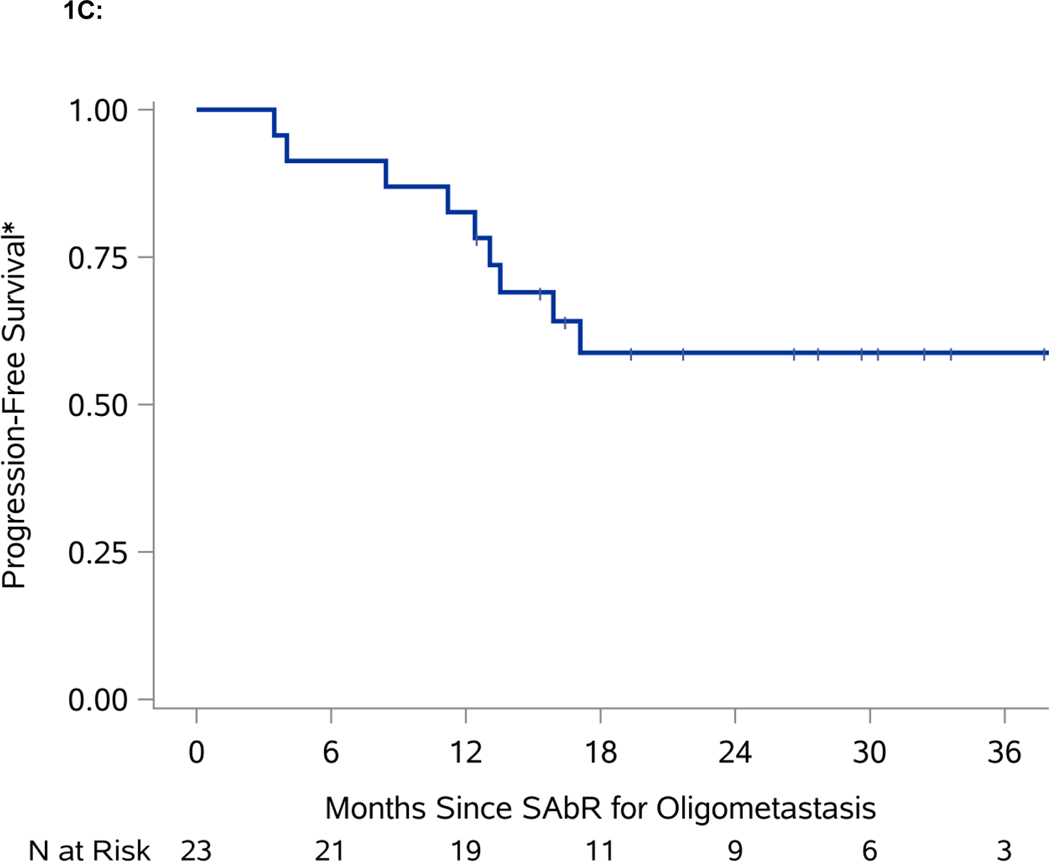
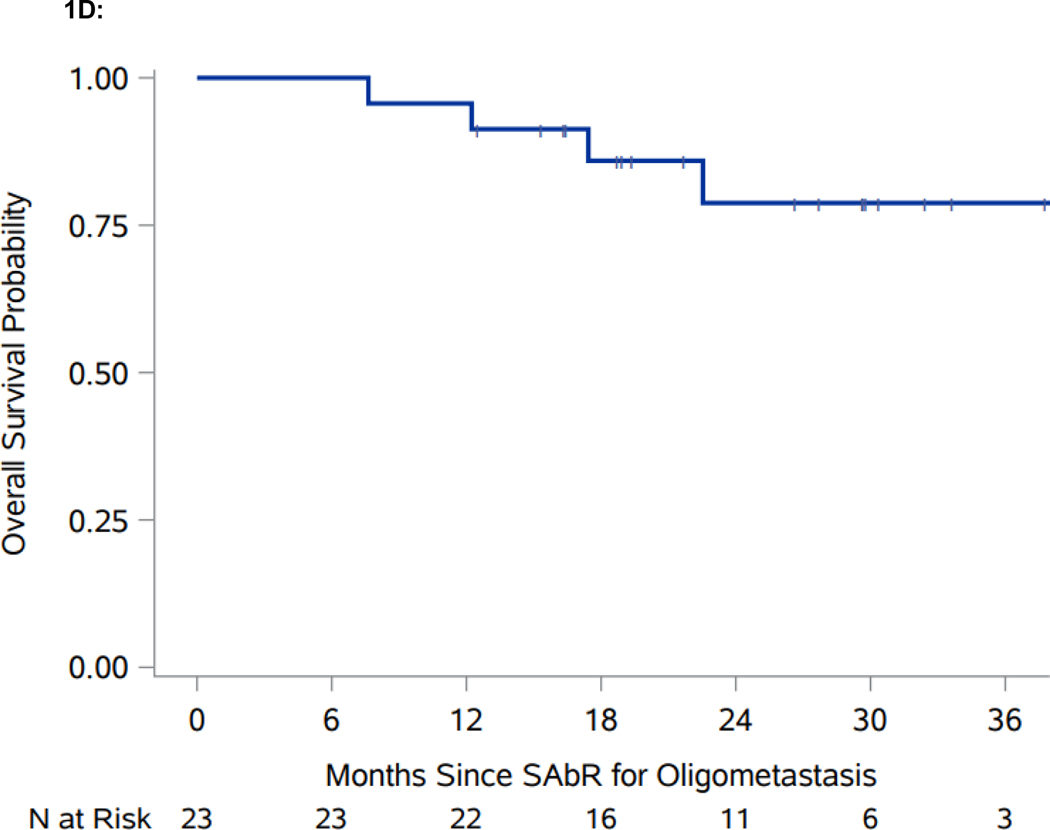
Outcome measurements and statistical analysis: This prospective phase II single-arm trial was powered to achieve a primary objective of freedom from systemic therapy for >1 yr in >60% of patients (using the Clopper and Pearson methodology). Secondary endpoints included progression-free survival (PFS), defined as the time from first SAbR to progression not amenable to SAbR (local failure at SAbR-treated sites, new metastases not amenable to SAbR, more than three new metastases, or brain metastases); patient-reported QOL metrics; local control (LC) rates; toxicity; cancer-specific survival (CSS); and overall survival (OS).
Results and limitations: Twenty-three patients received SAbR to 33 initial and 57 total sites. The median follow-up was 21.7 mo (interquartile range 16.3-30.3). Exceeding the prespecified 60% benchmark, freedom from systemic therapy at 1 yr was 91.3% (95% confidence interval [CI]: 69.5, 97.8). One-year PFS was 82.6% (95% CI: 60.1, 93.1). QOL was largely unaffected. LC was 100%. There were no grade 3/4 toxicities, but there was one death due to immune-related colitis 3 mo after SAbR while on subsequent checkpoint inhibitor therapy, where a SAbR contribution could not be excluded. One-year OS was 95.7% (95% CI: 72.9, 99.4); one-year CSS was 100%.
Conclusions: SAbR for oligometastatic RCC was associated with meaningful longitudinal disease control while preserving QOL. These data support further evaluation of SAbR for systemic therapy-naïve oligometastatic RCC.
Patient summary: Sequential stereotactic radiation therapy can safely and effectively control metastatic kidney cancer with limited spread for over a year without compromising patients' quality of life.
Keywords: Oligometastasis; Renal cell carcinoma; Stereotactic ablative radiotherapy; Stereotactic body radiation therapy; Stereotactic radiation.
Copyright © 2022 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Radiation Therapy for Renal Cell Carcinoma.Int J Radiat Oncol Biol Phys. 2023 Nov 1;117(3):523-525. doi: 10.1016/j.ijrobp.2023.03.073. Int J Radiat Oncol Biol Phys. 2023. PMID: 37739599 No abstract available.
References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209–49. Epub 2021/02/05. doi: 10.3322/caac.21660. PubMed PMID: 33538338. - DOI - PubMed
-
- Rabinovitch RA, Zelefsky MJ, Gaynor JJ, Fuks Z. Patterns of failure following surgical resection of renal cell carcinoma: implications for adjuvant local and systemic therapy. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 1994;12(1):206–12. - PubMed
-
- Motzer RJ, Tannir NM, McDermott DF, Aren Frontera O, Melichar B, Choueiri TK, Plimack ER, Barthelemy P, Porta C, George S, Powles T, Donskov F, Neiman V, Kollmannsberger CK, Salman P, Gurney H, Hawkins R, Ravaud A, Grimm MO, Bracarda S, Barrios CH, Tomita Y, Castellano D, Rini BI, Chen AC, Mekan S, McHenry MB, Wind-Rotolo M, Doan J, Sharma P, Hammers HJ, Escudier B, CheckMate I. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma. The New England journal of medicine. 2018;378(14):1277–90. Epub 2018/03/22. doi: 10.1056/NEJMoa1712126. - DOI - PMC - PubMed
-
- Rini BI, Plimack ER, Stus V, Gafanov R, Hawkins R, Nosov D, Pouliot F, Alekseev B, Soulieres D, Melichar B, Vynnychenko I, Kryzhanivska A, Bondarenko I, Azevedo SJ, Borchiellini D, Szczylik C, Markus M, McDermott RS, Bedke J, Tartas S, Chang YH, Tamada S, Shou Q, Perini RF, Chen M, Atkins MB, Powles T, Investigators K-. Pembrolizumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med. 2019;380(12):1116–27. Epub 2019/02/20. doi: 10.1056/NEJMoa1816714. - DOI - PubMed
-
- Motzer RJ, Penkov K, Haanen J, Rini B, Albiges L, Campbell MT, Venugopal B, Kollmannsberger C, Negrier S, Uemura M, Lee JL, Vasiliev A, Miller WH Jr., Gurney H, Schmidinger M, Larkin J, Atkins MB, Bedke J, Alekseev B, Wang J, Mariani M, Robbins PB, Chudnovsky A, Fowst C, Hariharan S, Huang B, di Pietro A, Choueiri TK. Avelumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med. 2019;380(12):1103–15. Epub 2019/02/20. doi: 10.1056/NEJMoa1816047. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
