

Diagnosis of paediatric tuberculosis by optically detecting two virulence factors on extracellular vesicles in blood samples
- PMID: 35986185
- PMCID: PMC9391224
- DOI: 10.1038/s41551-022-00922-1
Diagnosis of paediatric tuberculosis by optically detecting two virulence factors on extracellular vesicles in blood samples
Abstract
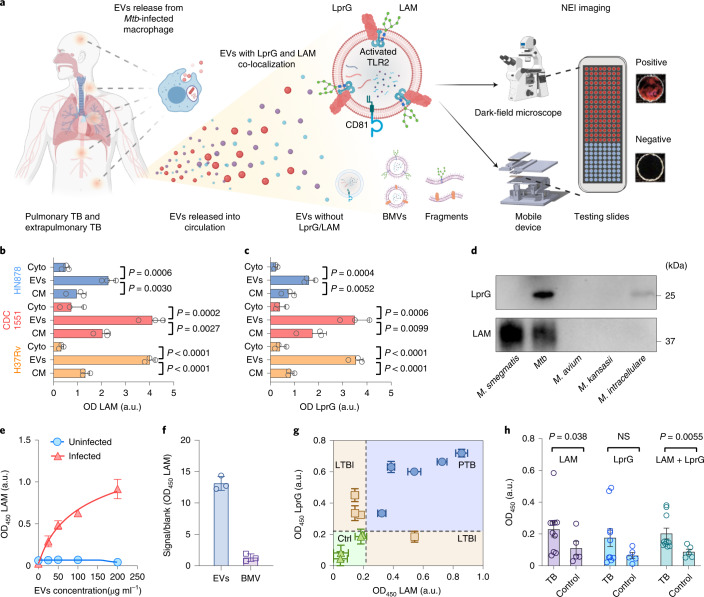
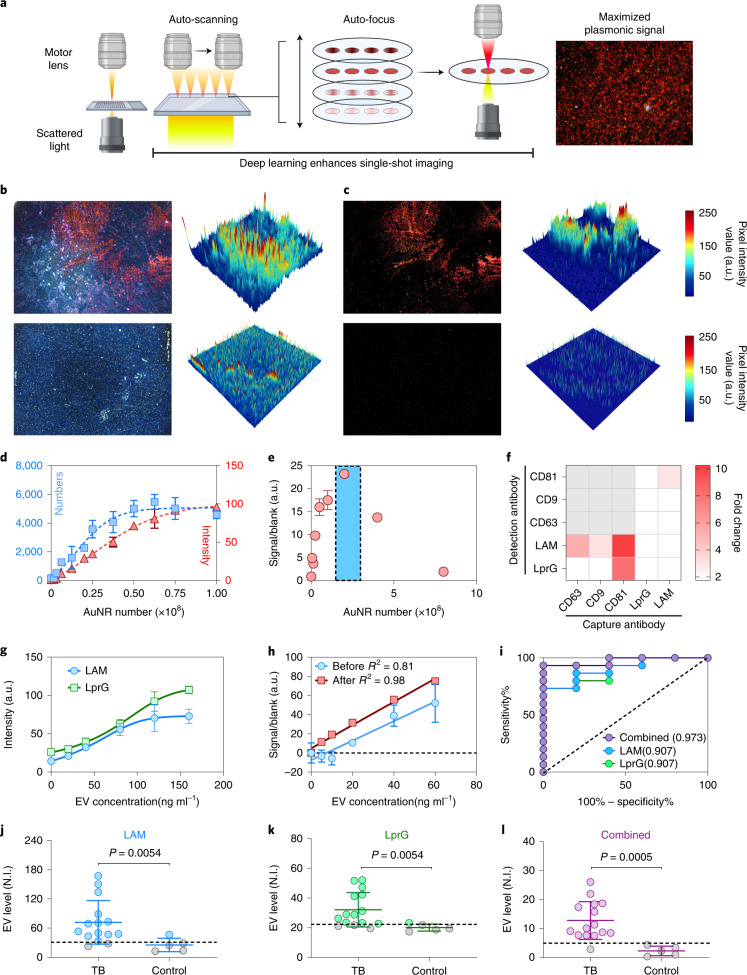
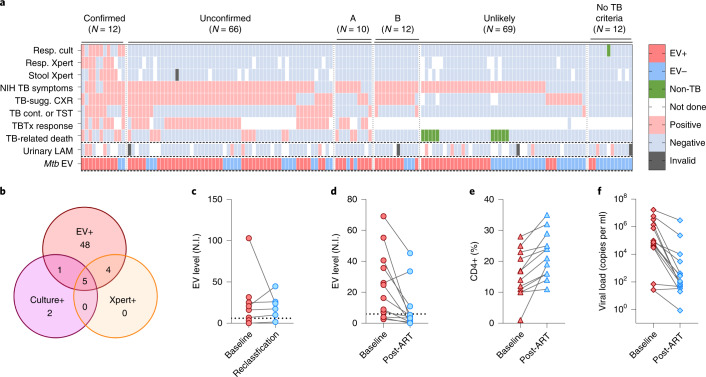
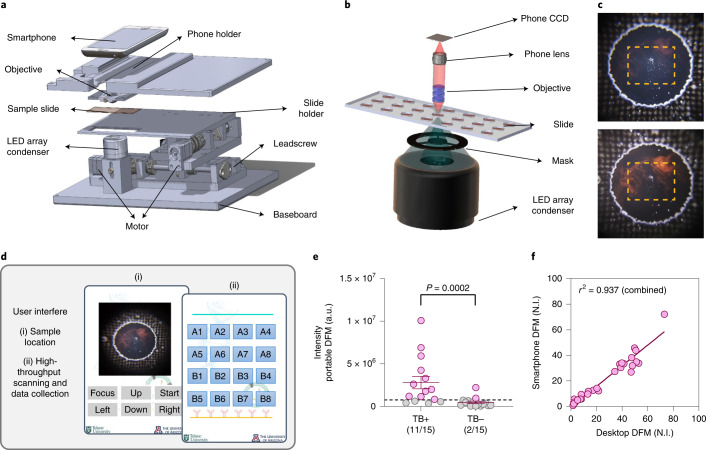
Sensitive and specific blood-based assays for the detection of pulmonary and extrapulmonary tuberculosis would reduce mortality associated with missed diagnoses, particularly in children. Here we report a nanoparticle-enhanced immunoassay read by dark-field microscopy that detects two Mycobacterium tuberculosis virulence factors (the glycolipid lipoarabinomannan and its carrier protein) on the surface of circulating extracellular vesicles. In a cohort study of 147 hospitalized and severely immunosuppressed children living with HIV, the assay detected 58 of the 78 (74%) cases of paediatric tuberculosis, 48 of the 66 (73%) cases that were missed by microbiological assays, and 8 out of 10 (80%) cases undiagnosed during the study. It also distinguished tuberculosis from latent-tuberculosis infections in non-human primates. We adapted the assay to make it portable and operable by a smartphone. With further development, the assay may facilitate the detection of tuberculosis at the point of care, particularly in resource-limited settings.
© 2022. The Author(s).
Conflict of interest statement
T.Y.H. and W.Z. have a provisional patent (‘Method of detecting TB in blood’) submitted through Tulane University. The rest of the authors declare no competing interests.
Figures
References
-
- Floyd K, Glaziou P, Zumla A, Raviglione M. The global tuberculosis epidemic and progress in care, prevention, and research: an overview in year 3 of the End TB era. Lancet Respir. Med. 2018;6:299–314. - PubMed
-
- Garrido-Cardenas J, de Lamo-Sevilla C, Cabezas-Fernández M, Manzano-Agugliaro F, Martínez-Lirola M. Global tuberculosis research and its future prospects. Tuberculosis. 2020;121:101917. - PubMed
-
- Harding E. WHO global progress report on tuberculosis elimination. Lancet Respir. Med. 2020;8:19. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 HD023412/HD/NICHD NIH HHS/United States
- R01 AI113725/AI/NIAID NIH HHS/United States
- U01 CA214254/CA/NCI NIH HHS/United States
- K23 AI120793/AI/NIAID NIH HHS/United States
- K23 AI143479/AI/NIAID NIH HHS/United States
- R01 HD090927/HD/NICHD NIH HHS/United States
- R01 AI134240/AI/NIAID NIH HHS/United States
- P51 OD011133/OD/NIH HHS/United States
- R01 HD103511/HD/NICHD NIH HHS/United States
- U42 OD010442/OD/NIH HHS/United States
- R01 AI162152/AI/NIAID NIH HHS/United States
- R01 AI122932/AI/NIAID NIH HHS/United States
- P51 OD011104/OD/NIH HHS/United States
- R21 NS130542/NS/NINDS NIH HHS/United States
- R01 AI144168/AI/NIAID NIH HHS/United States
- U54 GM104940/GM/NIGMS NIH HHS/United States
- R01 AI175618/AI/NIAID NIH HHS/United States
- U01 CA252965/CA/NCI NIH HHS/United States
- R21 AI143341/AI/NIAID NIH HHS/United States
- R01 AI134245/AI/NIAID NIH HHS/United States
- R03 AI140977/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
