

Achondroplasia in Latin America: practical recommendations for the multidisciplinary care of pediatric patients
- PMID: 35986266
- PMCID: PMC9389660
- DOI: 10.1186/s12887-022-03505-w
Achondroplasia in Latin America: practical recommendations for the multidisciplinary care of pediatric patients
Abstract
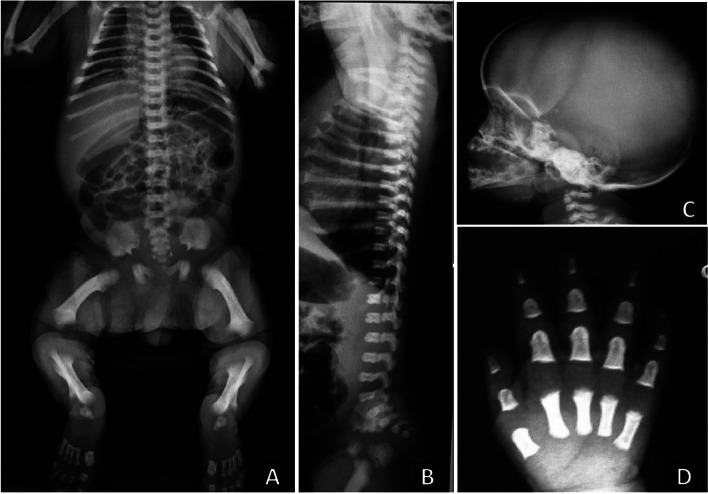
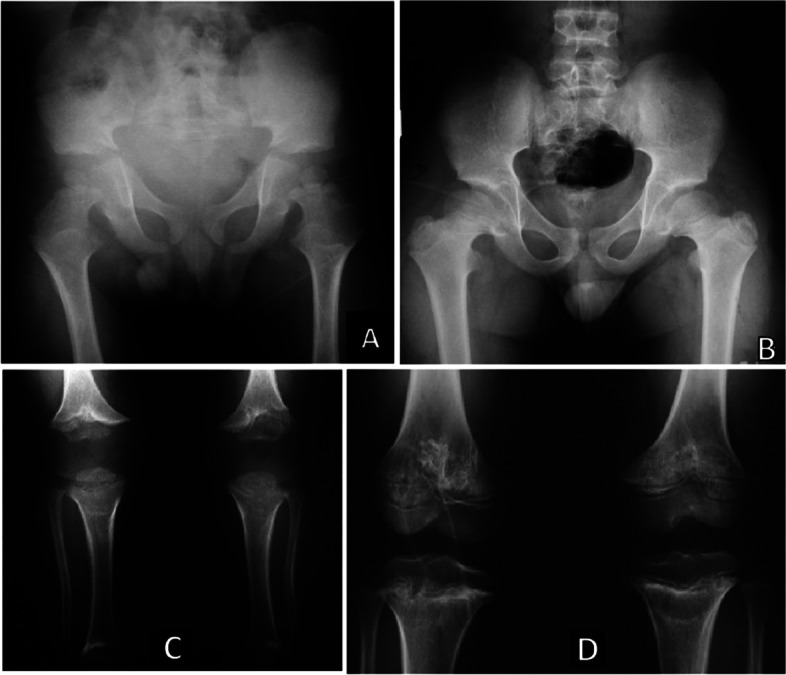
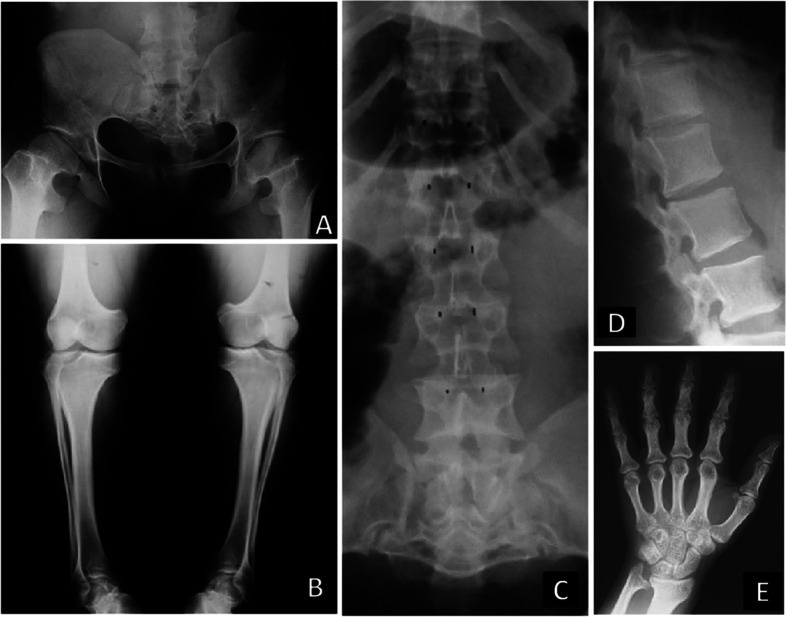
Background: Achondroplasia is the most common bone dysplasia associated with disproportionate short stature, and other comorbidities, such as foramen magnum stenosis, thoracolumbar kyphosis, lumbar hyperlordosis, genu varum and spinal compression. Additionally, patients affected with this condition have higher frequency of sleep disorders, ear infections, hearing loss and slowed development milestones. Considering these clinical features, we aimed to summarize the regional experts' recommendations for the multidisciplinary management of patients with achondroplasia in Latin America, a vast geographic territory with multicultural characteristics and with socio-economical differences of developing countries.
Methods: Latin American experts (from Argentina, Brazil, Chile and Colombia) particiáted of an Advisory Board meeting (October 2019), and had a structured discussion how patients with achondroplasia are followed in their healthcare centers and punctuated gaps and opportunities for regional improvement in the management of achondroplasia.
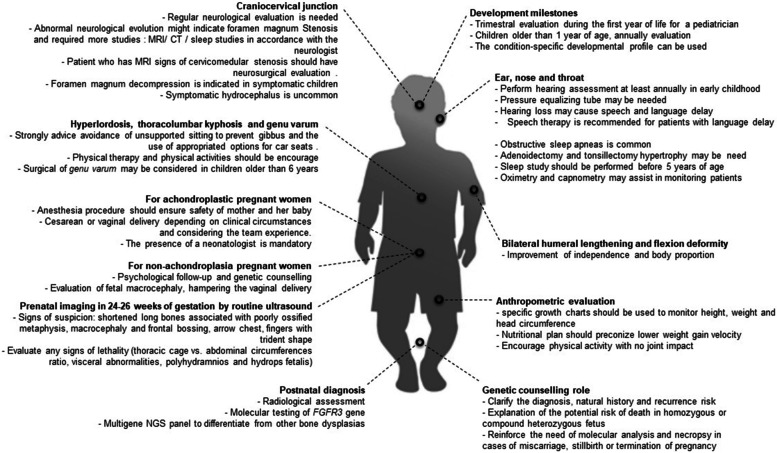
Results: Practical recommendations have been established for genetic counselling, prenatal diagnosis and planning of delivery in patients with achondroplasia. An outline of strategies was added as follow-up guidelines to specialists according to patient developmental phases, amongst them neurologic, orthopedic, otorhinolaryngologic, nutritional and anthropometric aspects, and related to development milestones. Additionally, the role of physical therapy, physical activity, phonoaudiology and other care related to the quality of life of patients and their families were discussed. Preoperative recommendations to patients with achondroplasia were also included.
Conclusions: This study summarized the main expert recommendations for the health care professionals management of achondroplasia in Latin America, reinforcing that achondroplasia-associated comorbidities are not limited to orthopedic concerns.
Keywords: Bone dysplasia; Dwarfism; FGFR3; Guideline; Management; Medical practice.
© 2022. The Author(s).
Conflict of interest statement
CAK, DB and NC received travel grant from BioMarin.
VF, PR, MDP, FA and WB received consulting honoraria and travel grant from BioMarin.
TF received grant from BioMarin, Ultragenyx and Alexion.
PFCS received consulting honoraria and travel grant from Pfizer, Novo Novordisk, Merck, BioMarin and Sandoz.
PFVM received consulting honoraria from BioMarin, research fellowship from Ultragenyx and travel grant from BioMarin and Ultragenyx.
JL received consulting honoraria and travel grant from BioMarin and Sanofi-Genzyme.
DC, ARB, NTR, FC, MCHR and CML declare no conflict of interest. All fees received by CML are donated to the CML Medical Foundation for Research and Genetic Diagnosis Support for families with unknown genetic disorders.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
