

Association between histological diaphragm atrophy and ultrasound diaphragm expiratory thickness in ventilated patients
- PMID: 35986366
- PMCID: PMC9392308
- DOI: 10.1186/s40560-022-00632-5
Association between histological diaphragm atrophy and ultrasound diaphragm expiratory thickness in ventilated patients
Abstract
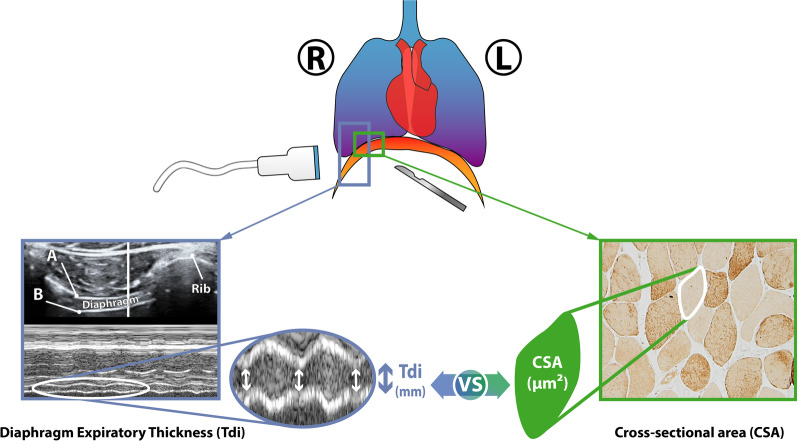
Background: Diaphragm fiber atrophy has been evidenced after short periods of mechanical ventilation (MV) and related to critical illness-associated diaphragm weakness. Atrophy is described as a decrease in diaphragm fiber cross-sectional area (CSA) in human diaphragm biopsy, but human samples are still difficult to obtain in clinics. In recent years, ultrasound has become a useful tool in intensive care to evaluate diaphragm anatomy. The present study aimed to evaluate the ability of diaphragm expiratory thickness (Tdi) measured by ultrasound to predict diaphragm atrophy, defined by a decrease in diaphragm fiber CSA obtained through diaphragm biopsy (the gold standard technique) in ventilated patients.
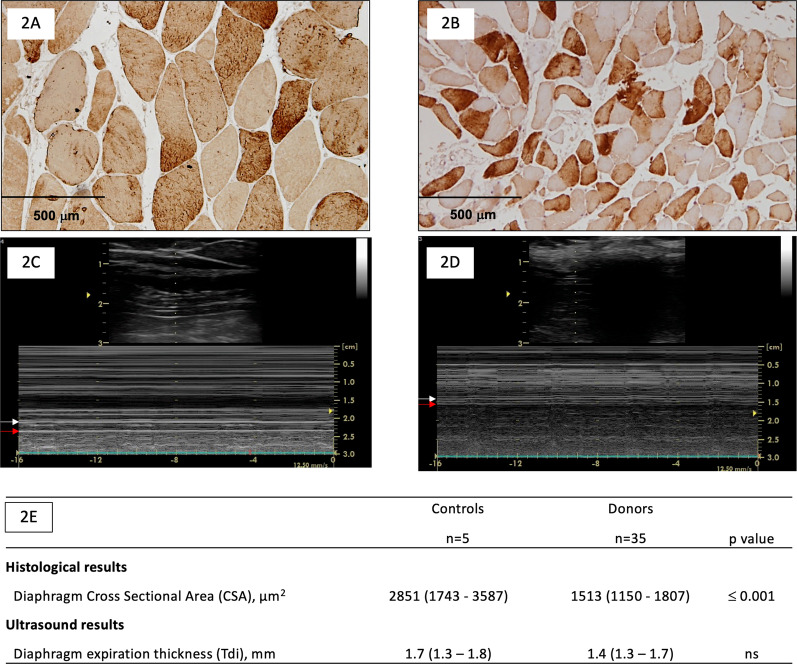
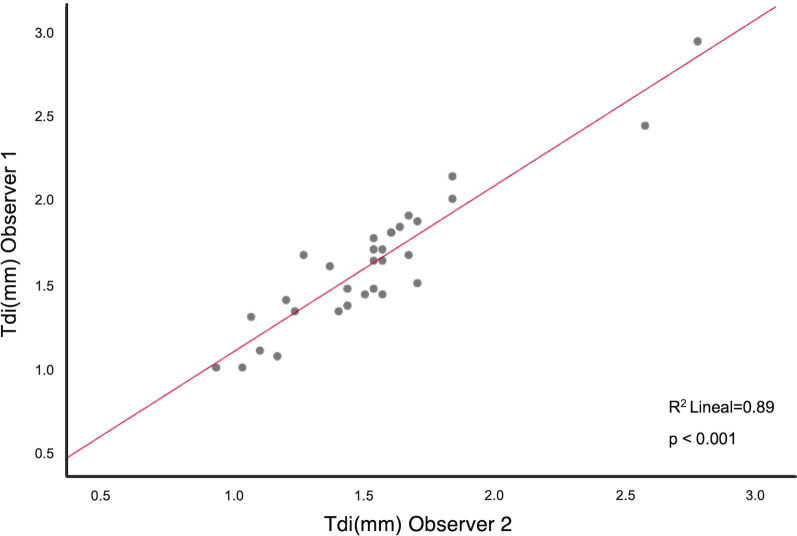
Methods: Diaphragm biopsies and diaphragm ultrasound were performed in ventilated donors and in control subjects. Demographic variables, comorbidities, severity on admission, treatment, laboratory test results and evolution variables were evaluated. Immunohistochemical analysis to determine CSA and ultrasound measurements of Tdi at end-expiration were performed, and median values of the control group were used as thresholds to determine agreement between them in further analysis. Sensitivity, specificity, and positive and negative predictive values of an ultrasound Tdi cutoff for detecting histologic atrophy were calculated. Agreement between two ultrasound observers was also assessed.
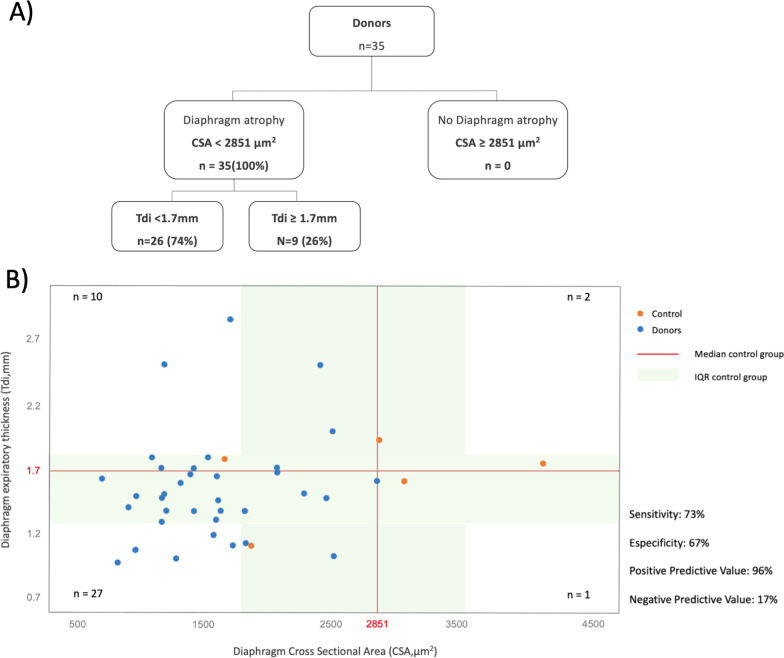
Results: Thirty-five ventilated organ donors and 5 ventilated controls were included, without differences in basic characteristics. CSA and Tdi were lower in donors than in controls. All donors presented lower CSA, but only 74% lower Tdi regarding control group thresholds. The cut-off value for lower diaphragm expiratory thickness (Tdi < 1.7 mm) presented a sensitivity of 73%, a specificity of 67%, a positive predictive value of 96% and a negative predictive value of 17% for determining the presence of diaphragm atrophy (CSA < 2851 μm2).
Conclusions: Diaphragm atrophy and thickness reduction is associated to MV. While a lower Tdi in diaphragm ultrasound is a good tool for diagnosing atrophy, normal or increased Tdi cannot rule atrophy out showing that both parameters should not be considered as synonymous.
Keywords: Atrophy; Critical illness-associated diaphragm weakness; Diaphragm thickness; Diaphragm ultrasound; Dysfunction; Muscle.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
