

DPP-4 inhibitors and GLP-1RAs: cardiovascular safety and benefits
- PMID: 35986429
- PMCID: PMC9392232
- DOI: 10.1186/s40779-022-00410-2
DPP-4 inhibitors and GLP-1RAs: cardiovascular safety and benefits
Abstract
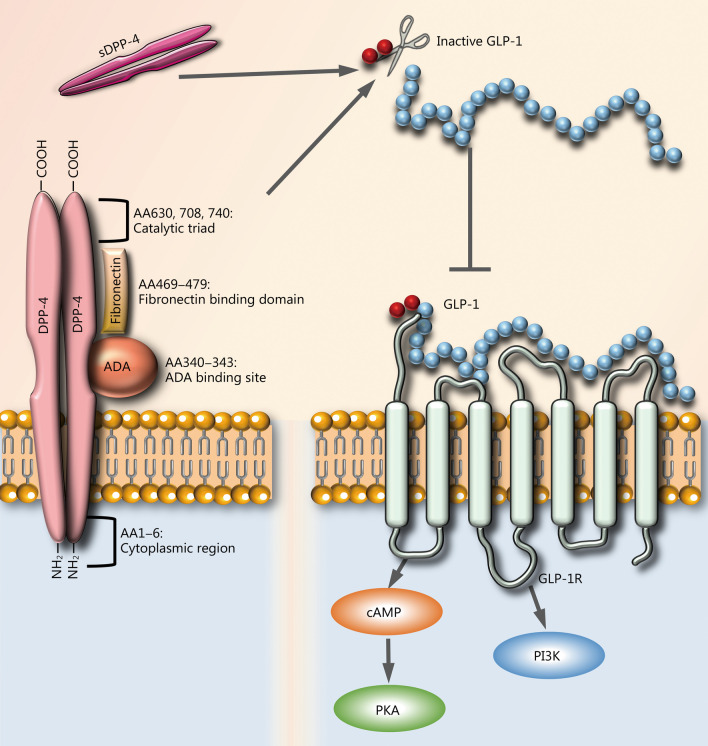
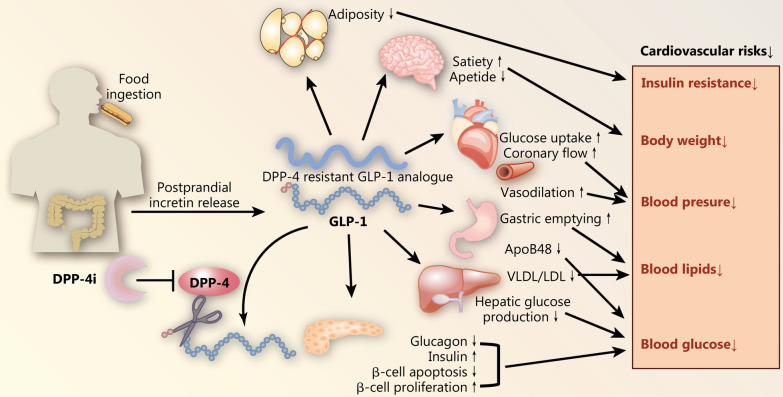
Glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors are commonly used treatments for patients with type 2 diabetes mellitus (T2DM). Both anti-diabetic treatments function by playing key modulatory roles in the incretin system. Though these drugs have been deemed effective in treating T2DM, the Food and Drug Administration (FDA) and some members of the scientific community have questioned the safety of these therapeutics relative to important cardiovascular endpoints. As a result, since 2008, the FDA has required all new drugs for glycemic control in T2DM patients to demonstrate cardiovascular safety. The present review article strives to assess the safety and benefits of incretin-based therapy, a new class of antidiabetic drug, on the health of patient cardiovascular systems. In the process, this review will also provide a physiological overview of the incretin system and how key components function in T2DM.
Keywords: Cardiovascular outcome; Dipeptidyl peptidase-4 inhibitors; Glucagon-like peptide-1 receptor agonists; Type 2 diabetes mellitus.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that there is no conflict of interest in this manuscript.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
